

Tetanus, an acute infectious disease, is highly prevalent worldwide, especially in developing countries. Due to respiratory failure and hemodynamic instability associated with dysautonomia, severe cases require intensive care, but little has been published regarding the management in the Intensive Care Unit.
ObjectiveTo draw a 10-year clinical–epidemiological profile of Intensive Care Unit patients with severe tetanus, observe their evolution in the Intensive Care Unit and identify risk factors for mortality.
MethodsIn this retrospective study, we used a standardized questionnaire to collect information from the records of patients with severe tetanus admitted to the intensive care unit of a referral hospital for infectious and contagious diseases in Northeastern Brazil.
ResultsThe initial sample included 144 patients, of whom 29 were excluded due to incomplete information, leaving a cohort of 115 subjects. The average age was 49.6±15.3 years, most patients had no (or incomplete) vaccination against tetanus, and most were male. The main intensive care-related complications were pneumonia (84.8%) and dysautonomia (69.7%). Mortality (44.5%) was higher than expected from the mean APACHE II score (11.8), with shock/multiple organ failure as the main cause of death (72.9%). The independent factors most predictive of mortality were APACHE II score, dysautonomia, continuous neuromuscular blockade and age.
ConclusionA high mortality rate was observed in our cohort of Intensive Care Unit patients with severe tetanus and a number of risk factors for mortality were identified. Our results provide important insights for the development of intervention protocols capable of reducing complications and mortality in this patient population.
Tetanus is a non-contagious acute infectious disease caused by exotoxins (tetanolysin and tetanospasmin) produced by Clostridium tetani. Despite being well documented since antiquity, tetanus remains an important cause of mortality worldwide. It is infrequently observed in developed countries but still represents a public health issue in developing nations.1–4
In severe cases the release of tetanolysin and tetanospasmin can lead to respiratory failure and hemodynamic instability associated with dysautonomia. The high doses of sedatives required to control muscle spams justify the frequent use of mechanical ventilation in the intensive care unit (ICU) setting. However, proper management can significantly reduce the risk of mortality.5–9
The literature provides few guidelines for the monitoring of ICU patients with severe tetanus. Management is currently based primarily on expertise. However, we believe the mortality rates observed in this patient population would be significantly reduced by the adoption of a carefully designed intervention protocol. The development of such a protocol requires further investigations into the clinical–epidemiological profile of ICU patients with severe tetanus in order to identify avoidable risk factors for mortality and subsidizing preventive measures.10
MaterialsThe study was based on information collected from non-electronic medical records and mechanical ventilation monitoring charts of patients with severe accidental tetanus admitted to the intensive care unit of a referral hospital for infectious and contagious diseases (Hospital São José de Doenças Infecciosas – HSJ) in Fortaleza, a state capital in Northeastern Brazil.
Patients under 18 years of age and patients with incomplete or illegible medical records and mechanical ventilation monitoring charts were excluded from the analysis.
The study protocol was approved by the HSJ Research Ethics Committee and filed under entry number CAAE #0053.0.042.000-08.
MethodsIn this retrospective and descriptive study, we analyzed a cohort of patients with severe tetanus admitted to the intensive care unit of HSJ between May 2003 and December 2013.
Using a questionnaire designed specifically for the study, three trained investigators collected patient information directly from non-electronic medical records at the hospital, covering the period from admission to discharge, transfer or death. Abstracted information included clinical–demographic data, intensive care data, and parameters potentially associated with mortality to be submitted to logistic regression. The patients were grouped according to outcome (death/survival).
Vaccination against tetanus was considered to be complete in patients who had received three doses of vaccine plus booster shots, as recommended by the National Immunization Service (PNI) of the Brazilian Ministry of Health (MoH).11 In patients with incomplete vaccination schedule, the time between the last vaccine shot and ICU admission could not be determined.
With regard to complications, dysautonomia included symptoms such as labile hypertension, tachycardia, heart rate irregularities, peripheral vasoconstriction, sweating, pyrexia, hypotension, and bradycardia, with no other obvious cause.12 Shock was defined as hypotension requiring vasoactive medication for more than 6h, except if dopamin was <5μg/mL. Acute renal failure was defined as a 1.5–2-fold increase, or a ≥0.3mg/dL increase, in serum creatinine levels in relation to baseline, or a <0.5mL/kg/h decrease in urinary output during 6h.13 Evidence of blood loss and need for transfusion were interpreted as bleeding. Pneumonia, atelectasis, pneumothorax, and obstructed tracheostomy were counted as complications if mentioned in the medical record.
In order to better evaluate severity, the respiratory data used in our analysis corresponded to the maximum values observed during mechanical ventilation.
Categorical variables were expressed as absolute and relative (percentage) frequencies while numerical variables were expressed as mean values±standard deviation. Continuous variables and their respective standard errors were tested with regard to distribution (skewness/kurtosis ratio) with the Kolmogorov–Smirnov test and the Shapiro–Wilk test.
Student's t test was used to compare means of two independent samples of variables with normal distribution. Pearson's chi-square test was used to verify compare dichotomous variables with non-normal distribution. Variables that did not satisfy Cochran's rule were analyzed with Fisher's exact test.
Variables of ICU patients with severe tetanus associated with mortality in univariate analysis were analyzed using a stepwise logistic regression model, calculating adjusted odds ratios and a 95% confidence intervals. The level of statistical significance (rejection of the null hypothesis) was set at 5% (p<0.05) in all tests.
In the logistic regression, “death of any cause” was the dependent variable while “APACHE II score”, “dysautonomia”, “continuous neuromuscular blockade” and “age” were used as independent variables.
The statistical analysis was performed with the software SPSS v. 19.0 (Statistical Package for the Social Sciences) for Windows.
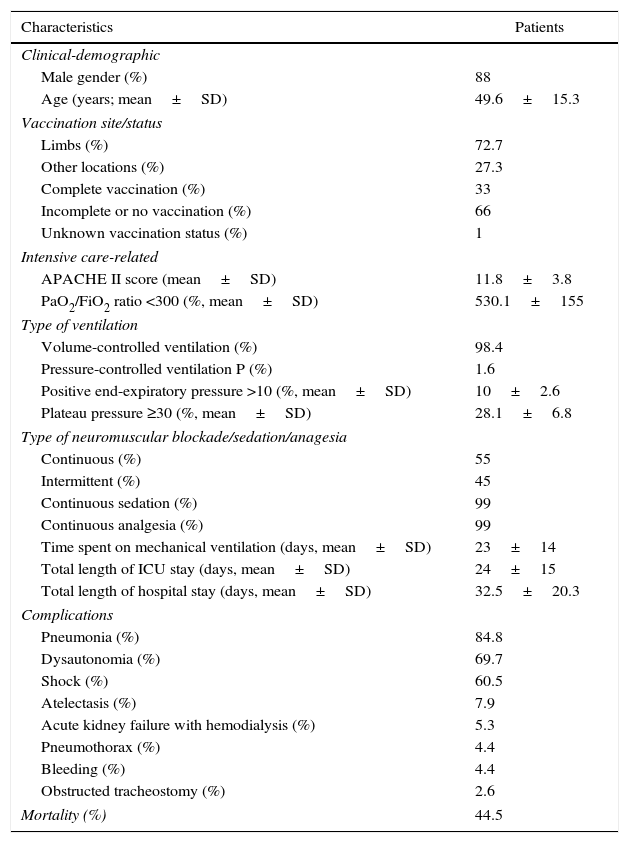
ResultsThe collected data of 144 patients are presented in Table 1. Twenty-nine subjects were excluded due to incomplete or illegible medical records, leaving a final cohort of 115 patients (Tables 2 and 3).
Characteristics of a cohort of 115 patients with severe accidental tetanus admitted to the intensive care unit of a referral hospital for infectious and contagious diseases in Fortaleza (Northeastern Brazil) between May 2003 and December 2013.
| Characteristics | Patients |
|---|---|
| Clinical-demographic | |
| Male gender (%) | 88 |
| Age (years; mean±SD) | 49.6±15.3 |
| Vaccination site/status | |
| Limbs (%) | 72.7 |
| Other locations (%) | 27.3 |
| Complete vaccination (%) | 33 |
| Incomplete or no vaccination (%) | 66 |
| Unknown vaccination status (%) | 1 |
| Intensive care-related | |
| APACHE II score (mean±SD) | 11.8±3.8 |
| PaO2/FiO2 ratio <300 (%, mean±SD) | 530.1±155 |
| Type of ventilation | |
| Volume-controlled ventilation (%) | 98.4 |
| Pressure-controlled ventilation P (%) | 1.6 |
| Positive end-expiratory pressure >10 (%, mean±SD) | 10±2.6 |
| Plateau pressure ≥30 (%, mean±SD) | 28.1±6.8 |
| Type of neuromuscular blockade/sedation/anagesia | |
| Continuous (%) | 55 |
| Intermittent (%) | 45 |
| Continuous sedation (%) | 99 |
| Continuous analgesia (%) | 99 |
| Time spent on mechanical ventilation (days, mean±SD) | 23±14 |
| Total length of ICU stay (days, mean±SD) | 24±15 |
| Total length of hospital stay (days, mean±SD) | 32.5±20.3 |
| Complications | |
| Pneumonia (%) | 84.8 |
| Dysautonomia (%) | 69.7 |
| Shock (%) | 60.5 |
| Atelectasis (%) | 7.9 |
| Acute kidney failure with hemodialysis (%) | 5.3 |
| Pneumothorax (%) | 4.4 |
| Bleeding (%) | 4.4 |
| Obstructed tracheostomy (%) | 2.6 |
| Mortality (%) | 44.5 |
SD, standard deviation.
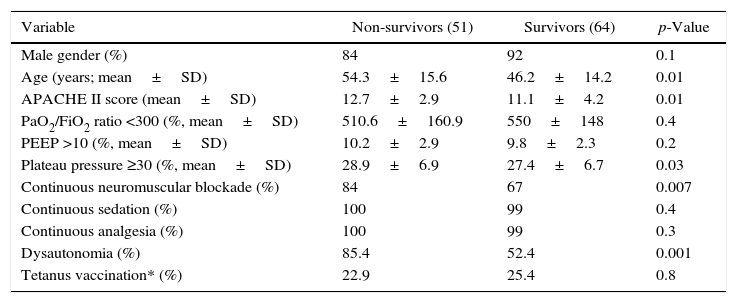
Factors associated with mortality in a cohort of 115 patients with severe accidental tetanus admitted to the intensive care unit of a referral hospital for infectious and contagious diseases in Fortaleza (Northeastern Brazil) between May 2003 and December 2013.
| Variable | Non-survivors (51) | Survivors (64) | p-Value |
|---|---|---|---|
| Male gender (%) | 84 | 92 | 0.1 |
| Age (years; mean±SD) | 54.3±15.6 | 46.2±14.2 | 0.01 |
| APACHE II score (mean±SD) | 12.7±2.9 | 11.1±4.2 | 0.01 |
| PaO2/FiO2 ratio <300 (%, mean±SD) | 510.6±160.9 | 550±148 | 0.4 |
| PEEP >10 (%, mean±SD) | 10.2±2.9 | 9.8±2.3 | 0.2 |
| Plateau pressure ≥30 (%, mean±SD) | 28.9±6.9 | 27.4±6.7 | 0.03 |
| Continuous neuromuscular blockade (%) | 84 | 67 | 0.007 |
| Continuous sedation (%) | 100 | 99 | 0.4 |
| Continuous analgesia (%) | 100 | 99 | 0.3 |
| Dysautonomia (%) | 85.4 | 52.4 | 0.001 |
| Tetanus vaccination* (%) | 22.9 | 25.4 | 0.8 |
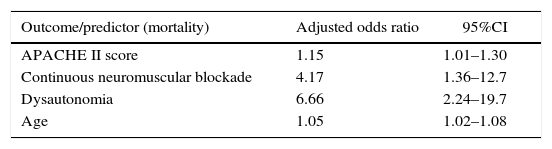
Logistic regression analysis of factors predictive of mortality in a cohort of 115 patients with severe accidental tetanus admitted to an intensive care unit in Fortaleza (Northeastern Brazil) between May 2003 and December 2013.
| Outcome/predictor (mortality) | Adjusted odds ratio | 95%CI |
|---|---|---|
| APACHE II score | 1.15 | 1.01–1.30 |
| Continuous neuromuscular blockade | 4.17 | 1.36–12.7 |
| Dysautonomia | 6.66 | 2.24–19.7 |
| Age | 1.05 | 1.02–1.08 |
PEEP, positive end-expiratory pressure; SD, standard deviation.
All ICU patients followed the same protocol during the first 24h after admission: surgical debridement of infected tissue, antibiotic therapy (metronidazole), and administration of immunoglobulin or anti-tetanus serum, as specified in the MoH guidelines in effect during the study period.10
In general, patients were discharged from the ICU shortly after weaning from mechanical ventilation.
During hospitalization, anticoagulation was predominantly maintained with unfractioned heparin at 5000UI every 8h (90% of the patients). Gastric protection was achieved with ranitidine (63.9%) or omeprazole (33.3%) or none (2.8%). Sedation and analgesia were induced with midazolam hydrochloride and fentanyl citrate, respectively. Due to the medical staff's familiarity with volume-controlled ventilation, this was by far the most frequently employed type of ventilation (98.4%), with average minimum and maximum flow volumes of 8.8mL/kg and 12.2mL/kg. The two patients who did not receive continuous sedation were kept on mechanical ventilation for short periods to protect the airways.
The most frequent non-pneumonia infections were related to the urinary tract (9%), blood stream (7%), or catheters (4%).
The main causes of death were shock/multiple organ failure (72.9%), respiratory failure/ARDS (15.3%), dysautonomia (3.4%), ventricular fibrillation (3.4%), gun shot wound confirmed by a coroner from the medical forensic institute (IML) (3.3%), and acute myocardial infarction (1.7%).
According to the logistic regression analysis each 1-point increase in the APACHE score corresponded to 1.15-fold increase in the mortality risk, and each 1-year increase in age increased 1.05-fold the risk of mortality. The risk of mortality was 4.17-fold higher for patients submitted to continuous neuromuscular blockade and 6.66-fold higher for patients with dysautonomia.
DiscussionThe size of our cohort of ICU patients with severe accidental tetanus was relatively large. Disregarding neonatal tetanus, 4104 cases of tetanus were registered in Brazil in the period 2003–2013, 315 of which in the state of Ceará (156 in the metropolitan region of Fortaleza).14 Nearly half (46%) of the cases reported in Ceará in this period required intensive care.
The final mortality rate in the present study was 44.5%. The variables significantly predictive of mortality in patients with severe tetanus were APACHE II score, continuous neuromuscular blockade, dysautonomia, and age.
APACHE II scores between six and 14 upon admission were associated with 8–15% mortality risk within the first 24h, a finding consistent with the results of other studies in which higher APACHE II scores were positively correlated with greater mortality.15,16 In our study, 84% of non-survivors received continuous neuromuscular blockade, suggesting a positive dose-dependent association with mortality. Other authors, such as Brauner (2002), have shown a significant association between mortality and exposure to high doses of blocking agents.17
Also in Brauner (2002), all patients developing dysautonomia died during the first or second week of hospitalization. It should be pointed out that pancuronium (which was administered in that study) can worsen tachycardia and hypertension, thus promoting dysautonomia.18 In the present study, dysautonomia was associated with increased mortality.
The mortality rate observed in this study was high compared to those of three other studies on severe tetanus in the ICU setting.15,17,18 This may be explained by intensive care-related morbidity and by the fact that vaccination was absent or incomplete in 66% of our cohort—a factor generally associated with greater severity and, hence, poorer prognosis and greater mortality.
Mortality rate tended to decrease slightly throughout the study period, especially from 2006 on. This may be explained by an overall improvement of the quality of local intensive care services available for patients with severe tetanus (Fig. 1).
 between May 2003 and December 2013.")
The length of hospitalization was comparable to that observed in other studies.15,17 Because severe tetanus affects multiple organs, including the autonomic nervous system, leading to dysautonomia and requires deep sedation, patients remain longer in the ICU and consequently are at greater risk for complications associated with prolonged mechanical ventilation.
Despite differences in plateau pressure between survivors and non-survivors, the variable was not a significant predictor of mortality in the multivariate analysis. In addition, in our cohort the incidence of pneumothorax was only 4.4%, which is similar to that reported by Brauner (2002) (3.6%).
Three decades ago, Trujillo (1987) reported similar results, but with low flow volumes,5 unlike the present study. Several other factors have been associated with tetanus-related barotrauma. Among these, prolonged mechanical ventilation and high positive end-expiratory pressure were observed in the present study, whereas ARDS, COPD, and necrotizing pneumonia were not.19 On the other hand, the use of higher flow volumes can help prevent atelectasis. The incidence of this complication was considerably lower in our cohort (7.9%) than in Brauner's (2002) (19%).20
The most frequent complications during hospitalization were pneumonia, dysautonomia, and shock, in line with findings in the literature.15,18 Despite improvements in the quality of intensive care, cardiovascular complications (including dysautonomia) are still frequent in patients with severe tetanus and high APACHE II scores. Due to the high risk of mortality from this type of complication, intensive hemodynamic monitoring is recommended.15,17–19 The high incidence of infectious complications may be explained by the prolonged ICU stay, invasive procedures, and prolonged use of mechanical ventilation.6
Prolonged use of mechanical ventilation may in part justify the high incidence of pneumonia (84.7%) during hospitalization, when compared to the incidence reported by Santos (2001) (57%).15 It may, however, also be related to the diagnostic criteria adopted in the study, based solely on the information provided in the medical records. In addition, during the study period covered by the, the ICU used no protocol or care bundle for the prevention of ventilator-associated pneumonia.
The extensive use of measures to prevent stress-related gastric ulcer and deep vein thrombosis, as observed in this study, rule out these conditions as causes of prolonged ICU stay and increased risk of hospital infection, especially in patients with associated risk factors.21–23
The male/female ratio in our cohort was approximately 9:1, confirming the predominance of the male gender in this condition. The difference in prevalence may be explained by the routine practice of vaccinating pregnant women against tetanus. The high average age in the cohort (49.6±15.3 years) shows that tetanus affects adults of productive age, with potentially significant socioeconomic impacts,15 especially in view of the fact that prognosis is worse in patients over 50 with accidental tetanus.24
The present study was limited by its retrospective design. Since all information was abstracted from medical records and charts filled out by different health professionals, there was no way of controlling for subjectivity in measurements and diagnosis.
The main cause of death was shock/multiple organ failure, although many such cases were likely secondary to infectious complications. Thus, it may be concluded that rigid control of intensive care-related infections and careful maintenance of hemodynamic stability should be regarded as priorities in management strategies for ICU patients with severe tetanus.
In conclusion, a high mortality was observed in our cohort of ICU patients with severe tetanus and a number of risk factors for mortality were identified. Our results provide important insights for the development of intervention protocols capable of reducing complications and mortality in this patient population.
Conflicts of interestThe authors declare no conflicts of interest.
