

Hepatitis C virus (HCV) infects B-lymphocytes, provokes cellular dysfunction and causes lymphoproliferative diseases such as cryoglobulinemia and non-Hodgkin's B-cell lymphoma. In the present study, we investigated the serum levels of kappa and lambda free light chains (FLC) of immunoglobulins and the kappa/lambda FLC ratio in Brazilian patients with chronic HCV infection and cryoglobulinemia. We also analyzed the immunochemical composition of the cryoglobulins in these patients. Twenty-eight cryoglobulinemic HCV patients composed the target group, while 37 HCV patients without cryoglobulinemia were included as controls. The median levels of kappa and lambda FLC were higher in patients with cryoglobulinemia compared to controls (p=0.001 and p=0.003, respectively), but the kappa/lambda FLC ratio was similar in patients with and without cryoglobulinemia (p>0.05). The median FLC ratio was higher in HCV patients presenting with advanced fibrosis of the liver compared to HCV patients without fibrosis (p=0.004). Kappa and lambda FLC levels were strongly correlated with the IgA, IgG and IgM levels in the patients with cryoglobulinemia. In patients without cryoglobulinemia, the kappa FLC level was only correlated with the IgG level, whereas the lambda FLC were weakly correlated with the IgA, IgG and IgM levels. An immunochemical pattern of mixed cryoglobulins (MC), predominantly IgM, IgG, IgA and kappa light chain, was verified in these immune complexes. We concluded that HCV-infected patients presenting cryoglobulinemia have vigorous polyclonal B-lymphocyte activation due to chronic HCV infection and persistent immune stimulation.
The chronic infection caused by hepatitis C virus (HCV) is characterized by both hepatic and extrahepatic clinical manifestations, and the latter are primarily caused by the ability of HCV to infect B lymphocytes. Mixed cryoglobulinemia (MC) and B-cell non-Hodgkin lymphoma (B-NHL) are among the main extrahepatic manifestations of chronic hepatitis C that are associated with lymphoproliferation. Cryoglobulins in chronic hepatitis C patients are cryoprecipitable immune complexes that contain IgM rheumatoid factor (IgM anti-IgG), HCV-RNA and core proteins associated with the IgG antibodies that are produced during the immune response of B-cells against HCV antigens. Interestingly, MC has been classified as a benign lymphoproliferative disorder that is observed in a substantial proportion of HCV-infected patients, but it can evolve to B-NHL. B-NHL is highly prevalent in chronic hepatitis C patients, but efficient HCV antiviral therapy causes the disappearance of the biomarkers that are associated with clonal lymphocyte activation and promotes the regression of some types of HCV-associated lymphomas.1–9
Recently, the serum levels of kappa and lambda free light chains (FLC) of immunoglobulin have been used to diagnose and monitor plasma cell dyscrasias and have been proposed as biomarkers of immune stimulation and inflammation.10,11 Serum FLC levels are determined by immunonephelometry using sheep polyclonal antibodies that recognize epitopes on free kappa and lambda chains, which are hidden when light and heavy chains are associated in the immunoglobulin molecule. Moreover, this sensitive immunoassay is able to detect very low concentrations of FLC (3–4mg/L) and is an effective substitute for immunofixation electrophoresis (IFE), which has an analytical sensitivity of only 100–150mg/L of FLC, for use in the diagnosis of B- and plasma cell dyscrasias.12,13
Patients who are chronically infected with HCV can present an increased level of FLC and a significant alteration in their FLC ratio, which has been associated with both MC and B-NHL.14,15 Although we have shown that Brazilian patients with chronic HCV infection present a high prevalence of cryoglobulinemia, no studies have been conducted to investigate markers of B-cell malignancies in these subjects.16,17
The aim of the present work was to investigate the serum levels of kappa and lambda FLC, the kappa/lambda FLC ratio, and the immunochemical composition of cryoglobulins in Brazilian patients with chronic HCV infection and cryoglobulinemia.
Materials and methodsPatientsSixty-five untreated HCV patients (29 women and 36 men) were included in this study. The presence of chronic HCV infection in these individuals was confirmed by clinical examination, positive anti-HCV serology, presence of serum HCV-RNA, and HCV genotyping. Clinical manifestations of mixed cryoglobulinemia, such as joint involvement, myalgias, fatigue, cutaneous vasculitis, renal immune-complex disease, or peripheral neuropathy were not observed in these subjects. Twenty healthy volunteers (10 men and 10 women) of similar ages were used to validate the international reference values used in the FLC determination. The Ethical Committee for Human Research of the Professor Edgard Santos Hospital approved the study.
Cryoglobulinemia and NOSACryoglobulinemia was assessed using tube and gel-diffusion cryoprecipitation18 (OKAZAKI et al., 1998). Serum levels of rheumatoid factor (normal value<20IU/mL) were determined by nephelometry (Immage immunochemistry system, Beckman-Coulter, Brea, CA, USA). Serum antinuclear antibody (ANA) and antibodies against smooth muscle (ASMA) and LKM1 antigen were tested using an indirect fluorescent antibody test (Viro-Immun, Labor-Diagnostika GmbH, Oberursel, Germany).
Liver histologyThe presence of liver fibrosis and liver necroinflammatory activity was ascertained in accordance with the METAVIR protocol.19
Free light chains (FLC)Serum levels of immunoglobulins were determined by nephelometry using the Immage immunochemistry system (Beckman-Coulter, USA). Serum levels of kappa and lambda free light chains (kappa and lambda FLC) were determined using the same method with Freelite® kits (The Binding Site, Birmingham, UK). The normal ranges for FLC were 3.3–19.4mg/L and 5.7–26.3mg/L for the kappa and lambda chains, respectively, whereas the normal range of the free kappa to lambda chain ratio was 0.3–1.65.20 These normal ranges were validated in 20 healthy individuals from the same population of HCV patients (99% CI: kappa FLC=10.85–15.05mg/L, lambda FLC=13.95–18.16mg/L and FLCr=0.71–0.92).
Immunofixation (IFE)The IMMUNOFIX® kit (The Binding Site, Birmingham, UK) was used to detect and identify the immunoglobulins and their light chains in solubilized cryoglobulins and to evaluate the presence of monoclonal immunoglobulins in this material.
Statistical analysisThe results were expressed as the mean±standard deviation (SD) or the median and interquartile range (IQR=Q1–Q3), in accordance with their distribution in the D’Agostino-Pearson test. The Mann–Whitney U test was used to compare the medians of two groups, whereas their means were compared using unpaired Student's t test. Correlation between two variables was assessed by the Spearman test, while the association between two categorical groups was analyzed using Fisher's exact test. The Prism 6.0 software from GraphPad (USA) was used for the statistical analyses, and the significance level was set at p<0.05.
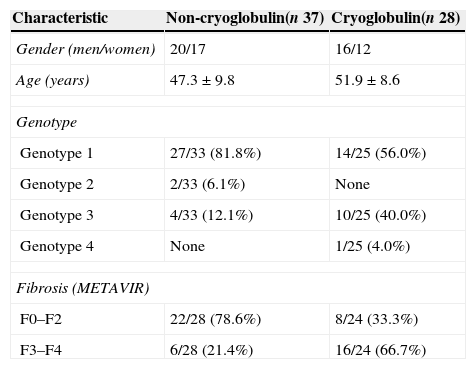
ResultsClinical and demographic characteristicsMost patients were infected with HCV genotype 1, followed in prevalence by infection with HCV genotype 3. HCV genotypes 2 and 4 were rarely observed. Serum cryoglobulinemia was observed in 43.1% (28/65) patients. Nineteen (67.9%) of these cryoglobulinemic individuals had positive rheumatoid factor (median 49.5IU/mL, IQR=24.0–104.0IU/mL), whereas significant levels of this autoantibody were found in 18 of the 37 (48.60%) patients without cryoglobulinemia (median=26.3IU/mL, IQR=22.6–41.3IU/mL) (p>0.05).
Three of the 65 (<10.0%) patients had antinuclear antibodies, whereas ASMA was detected in low titers in 28 (43.1%) patients. LKM1 antibodies were not found.
Liver fibrosis varied from F1 to F4 but was absent in one of the HCV-infected subjects. Sixteen of the 24 (66.7%) cryoglobulinemic patients had advanced fibrosis (F3–F4), while this condition was only observed in six of the 28 (21.4%) patients without cryoglobulinemia (p=0.002) (see Table 1).
Demographic, virologic, and clinical aspects of HCV-infected patients.
| Characteristic | Non-cryoglobulin(n 37) | Cryoglobulin(n 28) |
|---|---|---|
| Gender (men/women) | 20/17 | 16/12 |
| Age (years) | 47.3±9.8 | 51.9±8.6 |
| Genotype | ||
| Genotype 1 | 27/33 (81.8%) | 14/25 (56.0%) |
| Genotype 2 | 2/33 (6.1%) | None |
| Genotype 3 | 4/33 (12.1%) | 10/25 (40.0%) |
| Genotype 4 | None | 1/25 (4.0%) |
| Fibrosis (METAVIR) | ||
| F0–F2 | 22/28 (78.6%) | 8/24 (33.3%) |
| F3–F4 | 6/28 (21.4%) | 16/24 (66.7%) |
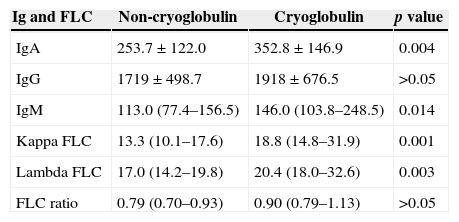
Cryoglobulinemic patients had higher levels of IgA and IgM than did patients without cryoglobulins (p=0.004 and p=0.014, respectively). However, no difference was observed in their IgG levels (p>0.05).
Patients with and without cryoglobulins differed in their median levels of kappa and lambda FLC (p=0.001 and p=0.003, respectively). A higher frequency of elevated kappa FLC levels was observed in patients with cryoglobulinemia (13/28, 46.4%) than in patients without cryoglobulins (7/37, 18.9%; p=0.029). The serum levels of kappa FLC were positively correlated with the serum levels of IgA (r=0.55, p=0.003), IgG (r=0.70, p<0.0001), and IgM (r=0.57, p=0.002) in cryoglobulinemic patients, whereas this correlation was observed only between the kappa FLC and IgG levels in patients without cryoglobulins (r=0.51, p=0.001). Similar correlations were observed between the serum levels of lambda FLC and IgA (r=0.61, p=0.001), IgG (r=0.67, p<0.0001) and IgM (r=0.62, p=0.001) in patients with cryoglobulinemia. These correlations were weaker in patients without cryoglobulins (IgA, r=0.37, p=0.026; IgG, r=0.52, p=0.001 and IgM, r=0.37, p=0.024).
Although the median FLC ratio was similar in the groups of patients with and without cryoglobulins (p>0.05) (see Table 2), two patients with cryoglobulins exhibited an increase in this ratio. The first had an FLC ratio of 1.79 (kappa FLC=66.30mg/L and lambda FLC=37.0mg/L), and the second had an FLC ratio of 3.51 (kappa FLC=196.6mg/L and lambda FLC=56.0mg/L). There was a positive correlation between the FLC ratio and the IgG level (r=0.54, p=0.003) and between the FLC ratio and the IgM level (r=0.38, p=0.048) in the cryoglobulinemic patient group. Although the median FLC ratio was higher in patients with advanced fibrosis (F3–F4) (p=0.004), it remained in the normal range (see Fig. 1).
Serum levels of immunoglobulins and kappa and lambda free light chains (FLC) in healthy control individuals and HCV-infected patients.
| Ig and FLC | Non-cryoglobulin | Cryoglobulin | p value |
|---|---|---|---|
| IgA | 253.7±122.0 | 352.8±146.9 | 0.004 |
| IgG | 1719±498.7 | 1918±676.5 | >0.05 |
| IgM | 113.0 (77.4–156.5) | 146.0 (103.8–248.5) | 0.014 |
| Kappa FLC | 13.3 (10.1–17.6) | 18.8 (14.8–31.9) | 0.001 |
| Lambda FLC | 17.0 (14.2–19.8) | 20.4 (18.0–32.6) | 0.003 |
| FLC ratio | 0.79 (0.70–0.93) | 0.90 (0.79–1.13) | >0.05 |
The immunoglobulin level is presented as the mean±SD (mg/dL) and the FLC as the median and IQR (mg/L).
 and advanced fibrosis (F3–F4). Horizontal lines represent the medians and interquartile range (25.0–75.0%). The normal FLC ratio range is 0.30–1.65.")
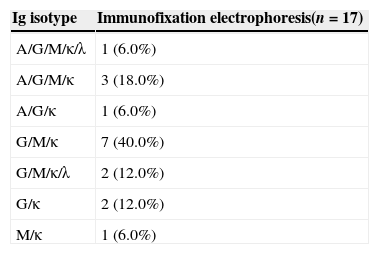
Immunofixation electrophoresis was performed in 17 solubilized cryoglobulin samples from the 28 patients with cryoglobulinemia (60.7%) who had enough material for this analysis. Fourteen cryoglobulins were immune complexes containing IgM, IgG and kappa light chain, and three had only one type of immunoglobulin (see Table 3).
DiscussionIn the present study, we investigated serum biomarkers of B-cell malignancy in Brazilian patients who were chronically infected with HCV. This virus infects and provokes dysfunction in B-lymphocytes, which is primarily associated with the production of cryoglobulin, NOSA, and B-NHL. Moreover, there is a well-documented association between persistent HCV infection and B-NHL that has been demonstrated by the high frequency of B-NHL in cryoglobulinemic patients and its regression following antiviral therapy.2–9
Confirming our previous reports, cryoglobulinemia was the main extrahepatic manifestation of HCV infection in Brazilian patients who participated of this study.16,17 Furthermore, we verified that cryoglobulinemic patients produced more IgA, IgM and both kappa and lambda FLC than did patients without cryoglobulinemia. In cryoglobulinemic individuals, the levels of both kappa and lambda FLC were strongly correlated with the IgA, IgG and IgM levels, suggesting an intense polyclonal production of these immunoglobulins. In contrast, a positive correlation was observed between the serum levels of kappa FLC and IgG in non-cryoglobulinemic HCV-infected patients. Furthermore, only a weak correlation was observed between serum levels of lambda FLC and levels of IgA, IgG and IgM in non-cryoglobulinemic HCV-infected patients. Although HCV infection causes persistent antigen stimulation and polyclonal activation, it is more vigorous in patients who produce cryoglobulins. Interestingly, this increase in both the FLC kappa and the FLC lambda did not alter FLC ratios of the patients, confirming its association with a polyclonal activation of B-lymphocytes and absence of B-cell malignancy.
Although we found an increased FLC ratio in two patients who had cryoglobulinemia and high serum levels of kappa and lambda FLC, this finding may be associated with the excessive production of immunoglobulins in these subjects.11
The FLC ratio was higher in HCV patients presenting advanced liver fibrosis. We had previously demonstrated that advanced stage of fibrosis in Brazilian patients is associated with cryoglobulinemia.21
Determination of the serum levels of kappa and lambda FLC, including the FLC ratio, is a valuable immunological tool for detecting the presence of polyclonal activation and monoclonal dyscrasias of B-lymphocytes and plasma cells.10,12,22 Although chronic HCV infection has been associated with B-malignancy, only two studies, both performed with French patients, investigated these biomarkers in cases of chronic hepatitis C. They demonstrated an increase of kappa FLC serum levels in patients with mixed cryoglobulinemia, observing an abnormal FLC ratio in patients with MC vasculitis and B-NHL, with a significant correlation between elevated FLC ratios and cryoglobulin level and severe HCV-related B-NHL.14,15 In contrast, FLC was shown to be a potential sensitive marker of polyclonal B-cell activation in a cohort of HIV-infected patients, who experienced increased risk of NHL.23
In our study, all HCV-infected patients with cryoglobulinemia were asymptomatic and did not have documentation of B-cell malignancy in their medical history. Thus, our observation of normal FLC ratios in these subjects is in accordance with one of the previous French studies that showed unaltered FLC ratios in patients with asymptomatic MC. Also in accordance with the results of the same French study, we observed a positive correlation between IgM and kappa FLC levels in these individuals.14 In contrast, we demonstrated that serum levels of kappa FLC were strongly correlated with IgA and IgG levels in patients with cryoglobulinemia. We also observed a strong correlation between lambda FLC levels and levels of IgA, IgG and IgM in these subjects. Nonetheless, the correlation of lambda FLC levels and the levels of these three immunoglobulins was also observed in patients without cryoglobulins, supporting the hypothesis that environmental and ethnic factors may cause the immunological differences observed between Brazilian and French patients with chronic HCV infection.
We did not verify a monoclonal pattern of IFE in the solubilized cryoglobulins from HCV-patients. These cryoprecipitable immune complexes were mainly formed by IgM plus IgG or IgA and kappa light chain, corresponding to type III mixed cryoglobulins.
In conclusion, most HCV cryoglobulinemic patients included in our study presented mixed cryoglobulins and a vigorous polyclonal activation of B-lymphocytes due to chronic HCV infection and persistent immune stimulation.
Conflicts of interestThe authors declare no conflicts of interest.
The National Council for Scientific and Technological Development (CNPq) and FAPESB supported this study. Ajax M. Atta, Raymundo Paraná and Maria Luiza B. Sousa Atta are recipients of CNPq-BPQ fellowships. Isabela. S. Oliveira and Larissa S. de Jesus are recipients of CAPES scholarships. Milena S. Cabral is the recipient of a FAPESB scholarship.
