


The aim of this study was to learn more about people diagnosed with acquired immunodeficiency syndrome (AIDS) at age 60 and above in Brazil, and to compare them with people diagnosed at a younger age.
MethodsThis study was based on the analysis of secondary data from the Brazilian AIDS Program. The study population consisted of people diagnosed with AIDS at age 60 and above. The comparison group was comprised of a 20% random sample of people diagnosed at age 18 to 59, frequency-matched by year of diagnosis.
Results544,846 cases of AIDS were reported in Brazil from 1980 until June 2009. Over 90% of cases were diagnosed between 18 and 59 years of age, and 13,657 (2.5%) at age 60 and above. The first case of AIDS among the elderly was reported in 1984. The comparison group consisted of 101,528 patients. Gender proportion was similar for both groups, and the proportion of people identified with AIDS after death in the Brazilian Mortality Information System (SIM) was 4% higher among the elderly. Both groups were also similar regarding the region of residence; a markedly higher proportion lived in Southeastern Brazil. Older people were more likely to have lower education and to have contracted AIDS by heterosexual contact, and less likely to be intravenous drug users. Male to female ratio among those diagnosed with AIDS at or above age 60 decreased over the years, in the same way as observed for the whole cohort. Mortality was higher among men in both groups. CD4 category (taken closest to the date of AIDS diagnosis) was very similar in both groups.
ConclusionThe characteristics of the epidemic among the elderly show similarities to the younger group considering gender distribution and CD4 category, but differ regarding educational level and exposure category. Also, the elderly were more likely not to have their AIDS condition promptly diagnosed.
According to the literature, prevalence and incidence of human immunodeficiency virus (HIV)/ acquired immunodeficiency syndrome (AIDS) at an older age is increasing: both as consequence of antiretroviral use, and because patients are becoming infected with HIV later in their lives.1–3
Statistics from the Centers for Disease Control and Prevention (CDC-USA) and from the Joint United Nations Program on HIV/AIDS (UNAIDS/WHO) also confirm the increasing numbers of AIDS in the elderly.4,5 Data from countries such as Brazil, Italy, England, Wales, Northern Ireland, and from other regions of Europe also corroborate this scenario.6–9 In Brazil, although still comprising a small proportion of cases, in the last few years there has been a trend of increase in cases aged 60 and above.10
There is still limited information regarding people diagnosed with AIDS at older age, especially when the World Health Organization's (WHO) definition of elderly for developing countries is considered (≥ 60 years old).
The paucity of information for this age bracket justified this study, aimed to describe the AIDS epidemic in Brazil among people diagnosed at age 60 and above, and to compare that incidence to those diagnosed from ages 18 to 59, and thus contribute to the implementation of appropriate actions by the National AIDS Program.
MethodsStudy designThis was an observational study based on the analysis of AIDS epidemic secondary data from the Brazilian AIDS Program. The Program works with information provided by four information systems: National Disease Notification System (Sistema de Informação de Agravos de Notificação – SINAN), Mortality Information System (Sistema de Informação sobre Mortalidade – SIM), Laboratory Exams Control System (Sistema de Controles de Informações Laboratoriais -SISCEL), and System for Logistic Control of Drugs (Sistema de Controle Logístico de Medicamentos -SICLOM). All information is stored in central databases, which were the sources used for this study.
In Brazil, AIDS notification is mandatory, and surveillance is based on notification of AIDS rather than HIV infection. The definition criteria used is based on a CD4 count below 350 cels/mm3, diagnosis of opportunistic diseases, or a score system for symptoms and laboratory parameters.
A unique key variable was created by database administrators from the Information and Epidemiologic Surveillance Unit of the National AIDS Program, allowing for a probabilistic record linkage for all databases.
Study populationThe databases contain data for all AIDS cases reported in Brazil from 1980 to June 2009. The main study population consisted of people aged 60 and above at the time of AIDS diagnosis. This age range was chosen based on the WHO definition for elderly in developing countries. People diagnosed at age 18 to 59 years old were used as a comparison group. A representative subsample of 20% was taken from the complete dataset of over 500,000 records. This subsample was frequency-matched by year of AIDS diagnosis, so that the samples represented the same time period of the epidemic. Another subsample (subsample 1) for those with available CD4 counts and antiretroviral use data was also evaluated (all diagnosed at age 60 and above, and a 20% random sample of those diagnosed at age 18 to 59 years, frequency-matched by year of diagnosis).
Analysis strategyData management and analysis were performed using the statistical package STATA, version 11. Descriptive analysis was performed using frequency distribution, means, medians, and histograms. The chi-squared test was used to analyze categorical variables, and Student's t-test was used to analyze quantitative variables. A significance level of 0.05 was considered.
Ethical approvalThe study was performed in accordance with Brazilian and international research ethics requirements; the project was approved by the Research Ethics Committee of the Universidade Federal de Minas Gerais (No. 0006.0.203.000-10) on February 2, 2010, by the Brazilian Research Ethics Commission on June 6, 2010 (No. 327/2010), and by the Research Ethics Commission of the London School of Hygiene and Tropical Medicine on May 7, 2010 (No. 009/223).
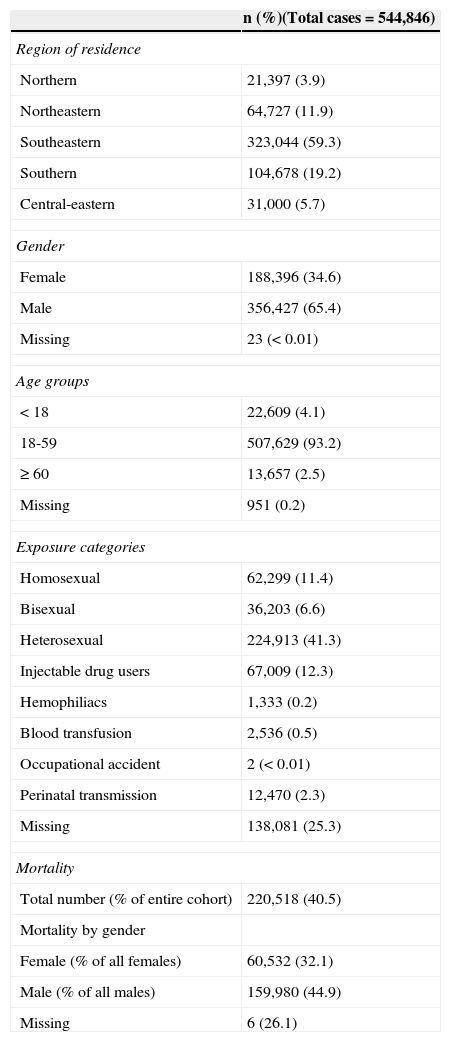
ResultsFrom 1980 to June 2009, 544,846 cases of AIDS were reported to the Brazilian Ministry of Health. The Southeastern Region accounted for almost 60% of the notifications. Over 90% were diagnosed from ages 18 to 59. The first case of AIDS among the elderly was reported in 1984, and the cumulative number of cases until June 2009 was 13,657, representing 2.5% of the entire AIDS cohort (Table 1), most of whom were diagnosed between 60 and 69 years of age (82%).
Cases of AIDS reported to the Brazilian Health Ministry (1980 to June 2009).
| n (%)(Total cases=544,846) | |
|---|---|
| Region of residence | |
| Northern | 21,397 (3.9) |
| Northeastern | 64,727 (11.9) |
| Southeastern | 323,044 (59.3) |
| Southern | 104,678 (19.2) |
| Central-eastern | 31,000 (5.7) |
| Gender | |
| Female | 188,396 (34.6) |
| Male | 356,427 (65.4) |
| Missing | 23 (< 0.01) |
| Age groups | |
| < 18 | 22,609 (4.1) |
| 18-59 | 507,629 (93.2) |
| ≥ 60 | 13,657 (2.5) |
| Missing | 951 (0.2) |
| Exposure categories | |
| Homosexual | 62,299 (11.4) |
| Bisexual | 36,203 (6.6) |
| Heterosexual | 224,913 (41.3) |
| Injectable drug users | 67,009 (12.3) |
| Hemophiliacs | 1,333 (0.2) |
| Blood transfusion | 2,536 (0.5) |
| Occupational accident | 2 (< 0.01) |
| Perinatal transmission | 12,470 (2.3) |
| Missing | 138,081 (25.3) |
| Mortality | |
| Total number (% of entire cohort) | 220,518 (40.5) |
| Mortality by gender | |
| Female (% of all females) | 60,532 (32.1) |
| Male (% of all males) | 159,980 (44.9) |
| Missing | 6 (26.1) |
The primary mode of transmission for the entire cohort was heterosexual contact (41.3%), followed by intravenous drug use, and homosexual contact, which contributed similarly (12.3% and 11.4%, respectively). Perinatal transmission contributed to 2.3% of notifications, and other exposure categories accounted for much lower notifications. However, these figures should be considered with caution, as the lack of information on mode of transmission is very high (25.3%) (Table 1).
Although the absolute numbers demonstrate a male predominance, an increase in the number of women reported over the years of the epidemic is evident. The first reported case among women occurred in 1983. The numbers rose to above 10% by the end of 1980s, increased to 20% in early 1990s, reached almost 30% of all cases notified in 1996, and peaked at 40% in 2002. Since then, this proportion has been maintained.
The cumulative number of deaths for the entire period is 220,518 (40.5%), and it is higher among males (44.9%) (Table 1). Mortality is higher in males of all ages, but the gap between males and females reduces with age. (Fig. 1)

In the first years of the epidemic, a fluctuation in the proportion of cases in older people was probably due to the small number of notifications; it has increased gradually from less than 2% before 1998, reached 3% in 2004, and is almost 4% in recent years (Fig. 2).
.")
Of all cases of AIDS diagnosed in elderly people, 65.6% (8,959) occurred among men. The mean age was similar for males and females (65.5±5.2 vs. 65.2±5.1, respectively).
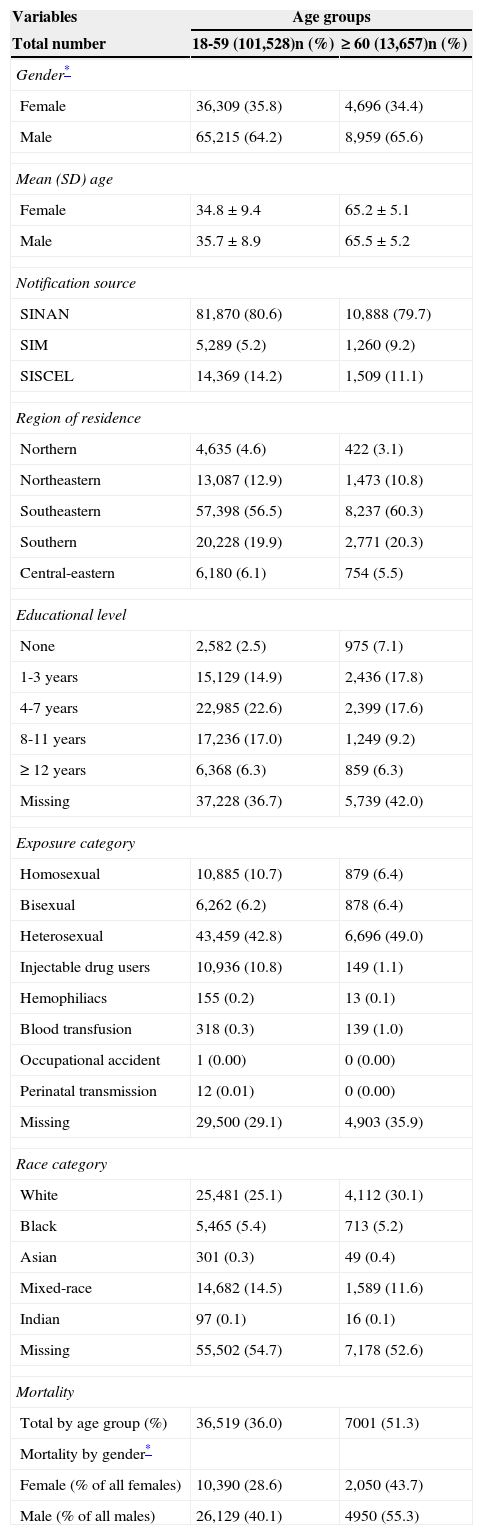
The comparative group consisted of 101,528 people. Gender structure was similar in both groups, and the proportion of people identified with AIDS after death (according to data obtained from the SIM) was 4% higher among the elderly group. Both groups were also similar regarding region of residence, which was markedly higher in the Southeastern Region, followed by the Southern Region; together, these two regions comprised almost 80% of the reported cases (Table 2).
Characteristics of those diagnosed at an old age compared to a 20% subsample of those diagnosed at 18 to 59 years.
| Variables | Age groups | |
|---|---|---|
| Total number | 18-59 (101,528)n (%) | ≥ 60 (13,657)n (%) |
| Gender* | ||
| Female | 36,309 (35.8) | 4,696 (34.4) |
| Male | 65,215 (64.2) | 8,959 (65.6) |
| Mean (SD) age | ||
| Female | 34.8±9.4 | 65.2±5.1 |
| Male | 35.7±8.9 | 65.5±5.2 |
| Notification source | ||
| SINAN | 81,870 (80.6) | 10,888 (79.7) |
| SIM | 5,289 (5.2) | 1,260 (9.2) |
| SISCEL | 14,369 (14.2) | 1,509 (11.1) |
| Region of residence | ||
| Northern | 4,635 (4.6) | 422 (3.1) |
| Northeastern | 13,087 (12.9) | 1,473 (10.8) |
| Southeastern | 57,398 (56.5) | 8,237 (60.3) |
| Southern | 20,228 (19.9) | 2,771 (20.3) |
| Central-eastern | 6,180 (6.1) | 754 (5.5) |
| Educational level | ||
| None | 2,582 (2.5) | 975 (7.1) |
| 1-3 years | 15,129 (14.9) | 2,436 (17.8) |
| 4-7 years | 22,985 (22.6) | 2,399 (17.6) |
| 8-11 years | 17,236 (17.0) | 1,249 (9.2) |
| ≥ 12 years | 6,368 (6.3) | 859 (6.3) |
| Missing | 37,228 (36.7) | 5,739 (42.0) |
| Exposure category | ||
| Homosexual | 10,885 (10.7) | 879 (6.4) |
| Bisexual | 6,262 (6.2) | 878 (6.4) |
| Heterosexual | 43,459 (42.8) | 6,696 (49.0) |
| Injectable drug users | 10,936 (10.8) | 149 (1.1) |
| Hemophiliacs | 155 (0.2) | 13 (0.1) |
| Blood transfusion | 318 (0.3) | 139 (1.0) |
| Occupational accident | 1 (0.00) | 0 (0.00) |
| Perinatal transmission | 12 (0.01) | 0 (0.00) |
| Missing | 29,500 (29.1) | 4,903 (35.9) |
| Race category | ||
| White | 25,481 (25.1) | 4,112 (30.1) |
| Black | 5,465 (5.4) | 713 (5.2) |
| Asian | 301 (0.3) | 49 (0.4) |
| Mixed-race | 14,682 (14.5) | 1,589 (11.6) |
| Indian | 97 (0.1) | 16 (0.1) |
| Missing | 55,502 (54.7) | 7,178 (52.6) |
| Mortality | ||
| Total by age group (%) | 36,519 (36.0) | 7001 (51.3) |
| Mortality by gender* | ||
| Female (% of all females) | 10,390 (28.6) | 2,050 (43.7) |
| Male (% of all males) | 26,129 (40.1) | 4950 (55.3) |
There was a significant difference in the educational level between the two groups; older people were more likely to have lower educational levels. Also, there was a large amount of missing data on education for both age groups (p < 0.01).
There was a significant difference in HIV exposure categories; older people were more likely to have contracted AIDS by heterosexual contact, and less likely to be intravenous drug users. There was a large amount of missing data for both age groups, higher among the older group (p < 0.01).
Regarding ethnicity, there was a high proportion of white and a low proportion of mixed-race among the elderly, but missing data reached more than 50% in both groups (Table 2).
Male to female ratio among those diagnosed at age 60 or above decreases over the years; the same was observed for the entire cohort. In 1986, the ratio was 19:1, it decreased to 7:1 in 1990, reaching 1.9:1 in 2000 and 1.5:1 in 2008.
Mortality among the elderly for the entire period was 15% higher than among the young (Table 2). The total number of deaths was higher for men in both age groups.
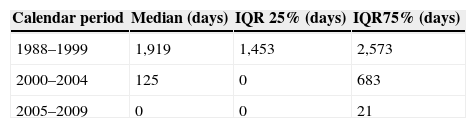
Information on CD4 count and/or antiretroviral use was available for 6,869 (50.3%) of those diagnosed at age 60 years and above, and for 281,074 (55.4%) of those diagnosed between ages 18 to 59 years. Until 1995, only 20% of all reported patients had this information available, increasing to 50% in 1998, and to 80% or more after 2005, which represents those who were diagnosed later in the epidemic. It can be also observed that time between CD4 count and date of diagnosis varied by period, with longer gaps for those diagnosed earlier in the epidemic (Table 3).
Overall, baseline characteristics for those with available laboratory and antiretroviral data (subsample 1) were very similar compared to the subsample used to compare all people aged 60 and above with those younger. A slight increase in the proportion of females, heterosexuals, and whites was observed in both groups, but a similar distribution within each group was maintained when compared to subsample1.
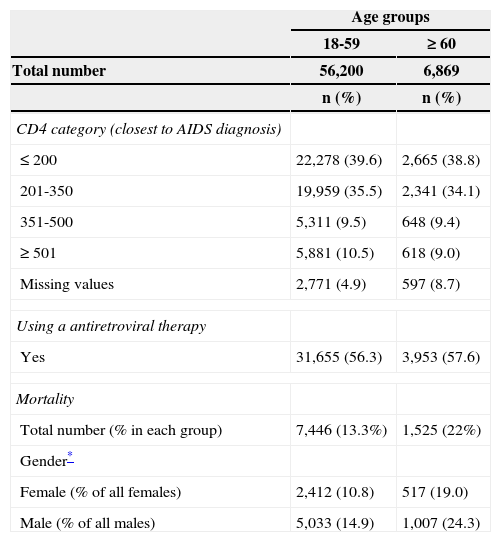
Considering CD4 category (closest to the date of AIDS diagnosis) the distribution was similar for both groups. Over 70% cases in both groups had CD4 lower than 350; of these, approximately 40% had a CD4 count lower than 200 cells/mm3. CD4 count was available for 59,701 subjects (95%). The proportion with missing CD4 counts was higher in the elderly group (9% and 5%, respectively) (Table 4). Median time between date of AIDS diagnosis and date of closest CD4 exam was six days (IQR=0 to 342 days); for 25% this median time is zero and for 75% it is 342 days. The median time for the closest CD4 was very similar in both groups and also for both genders. Antiretroviral use was also similar.
Characteristics of CD4, antiretroviral use and mortality among those diagnosed at older age compared to the young group.
| Age groups | ||
|---|---|---|
| 18-59 | ≥ 60 | |
| Total number | 56,200 | 6,869 |
| n (%) | n (%) | |
| CD4 category (closest to AIDS diagnosis) | ||
| ≤ 200 | 22,278 (39.6) | 2,665 (38.8) |
| 201-350 | 19,959 (35.5) | 2,341 (34.1) |
| 351-500 | 5,311 (9.5) | 648 (9.4) |
| ≥ 501 | 5,881 (10.5) | 618 (9.0) |
| Missing values | 2,771 (4.9) | 597 (8.7) |
| Using a antiretroviral therapy | ||
| Yes | 31,655 (56.3) | 3,953 (57.6) |
| Mortality | ||
| Total number (% in each group) | 7,446 (13.3%) | 1,525 (22%) |
| Gender* | ||
| Female (% of all females) | 2,412 (10.8) | 517 (19.0) |
| Male (% of all males) | 5,033 (14.9) | 1,007 (24.3) |
Mortality was much lower among those with information on CD4 count and/or antiretroviral use, in both groups. In the younger group, overall mortality was 13.3% vs. 81% among those without information. However, mortality was still higher in males than in females (Table 4).
DiscussionThe present study aimed at bringing information on a still unknown territory of the AIDS scenario, that of people diagnosed later in life.
The AIDS epidemic in Brazil is concentrated in vulnerable groups (mainly homosexual men, injectable drug users, and sex workers), with predominance of males and of people diagnosed between ages 18 to 49. There is a trend towards more women being diagnosed from the start of the epidemic until recent years. Although the possibility of delay in notification and underreporting should be considered, it is interesting to note that since 2002, the male to female ratio has stabilized at around 2:1. A substantial proportion of the entire cohort has already died, and mortality is higher among males in all age groups.
From all notifications, 10.7% and 4.5% were recovered from the SISCEL/SICLOM and SIM databases, respectively, reinforcing the usefulness of the database linkage approach. Since 2004, the Brazilian AIDS Program has been using the record linkage method between the databases to identify duplicities and underreporting of AIDS cases. This measure improves the quality of information and epidemiological analysis, contributing to a better understanding of the epidemic and guiding the preventive and control measures.
People diagnosed over age 60 in Brazil have been diagnosed later in the epidemic, and despite still constituting a small proportion of the cohort, they present a progressive rise, particularly in recent years, while a trend towards stability in number of notifications is observed for all other age ranges.10 This group is similar to the comparison group regarding gender distribution and region of residence, but have lower educational level and were less likely to have been infected by intravenous drug use; heterosexual contact was the most prevalent route of transmission. Pratt et al. in the UK11 and Navarro et al. in Spain12 also reported a predominance of men in their studies among people aged 60 and above and 50 and above, respectively. Navarro et al. also found a lower proportion of intravenous drug users.12 Longo et al. in Italy showed similar findings, a lower proportion of homosexuals and intravenous drug users among those diagnosed at age 60 and above, compared to those diagnosed at ages 50 to 59.7
Although most of the studies use a different definition for elderly (≥ 50 years), a trend towards increasing number of AIDS cases diagnosed among elderly in recent years is also reported by Lazarus et al.,9 Longo et al.,7 and Smith et al.8 Data from the CDC regarding people aged 60 and above concur with these studies.5 These data signalize a new profile of the AIDS epidemic in the world, the “ageing” of the AIDS epidemic, with the expected associations of other related and unrelated chronic illnesses.
Compared to the younger group, the proportion of those diagnosed after death (by SIM database) in this study was higher (9.2% vs. 4.4%), suggesting they were more likely not to have had their condition diagnosed on time. A lower level of diagnostic suspicion among the elderly has been reported, leading to missing or late diagnosis, which has impact on patients’ prognosis. However, using CD4 count ≤ 200 as a proxy for late diagnosis in this study, a similar proportion was found for both groups. As the CD4 count at the exact time of AIDS diagnosis was not available for all cases, the result closest to date of diagnosis was considered. This approach appears reasonable, given that the median time was six days from diagnosis, and that 75% of the sample CD4 counts were available within one year of diagnosis.
Another important point to discuss in the context of AIDS diagnosed at an older age is survival. The mortality rate observed among people diagnosed at 60 years and above was very high, considering that these patients were diagnosed in a more recent period of the epidemic. Given that they were diagnosed with a similar level of immunodeficiency (CD4 < 200) as the younger group it is possible that other health conditions were associated, which reinforces the need to remind health professionals to also offer HIV testing to their elder patients.
Mortality rate was even higher in males, and this also holds true in the analysis of age subgroups, including those diagnosed from ages 18 to 59. This finding is similar to data from the Brazilian AIDS Program: AIDS mortality has always been higher in men, but it has been decreasing with time and more pronouncedly when compared with women. It reduced from 15.1/100,000 in 1995 to 8.2 in 2007, while the reduction observed for women was from 4.8/100,000 in 1996 to 3.9 in 2007.10 Saraceni et al. showed a significant decrease in mortality in Rio de Janeiro (Brazil) after the introduction of antiretroviral therapy. The decrease was observed for both genders, but it was more significant for males. Mortality was also higher for those with lower education level, among those diagnosed from ages 20 to 49 years, and a trend towards increasing mortality was observed in those diagnosed at ages 50 and above.13
Limitations of the studyThis study relies on analysis of secondary data on reported AIDS cases in Brazil. Even though it is time saving, less expensive, and useful for decision-making managers, some disadvantages must be considered. The database sources came from routine epidemiologic surveillance and were not designed to address a specific hypothesis. Thus, important information could not be evaluated, and potential confounders such as co-morbidities, opportunistic infections presented at the time of diagnosis of AIDS, and smoking habits could not be controlled.
Although the AIDS case report form is the same for the entire country and is completed by health professionals, the quality of reporting and completeness of information need to be improved. A study conducted in Brazil in 2005 evaluating the consistency and completeness of information in the SINAN database has identified an improvement in case reporting over the years, but found a high amount of missing information related to socio-demographic and epidemiologic variables. The present study confirmed these findings.
Delay in reporting cases also constitutes a limitation and can affect analysis of recent periods of the epidemic. Underreporting of cases has been improved since the linkage of databases approach was implemented by the National AIDS Program, as shown by Fonseca and Bastos.14
Regarding HIV exposure variables, differential misclassification should be considered. For instance, if older people were less likely than younger people to admit homosexuality and drug use, this would bias the estimate of exposure category.
Considering the epidemic overall, results cannot be generalized, as there was over 50% of unavailable data on CD4 and antiretroviral use. Conversely, since data completeness has improved, the results are more reliable for the more recent period of the epidemic.
ConclusionsThis study corroborates the literature regarding the ageing of the AIDS epidemic. In this cohort the main characteristics among elderly were similar to the comparison groups.
Completeness of information is a point that must be addressed in the Brazilian epidemic.
Although many questions remain to be investigated and understood in the HIV/AIDS scenario among the elderly in order to implement prevention and control measures, the following recommendations may be proposed:
- •
Strengthening and maintenance of HIV/AIDS awareness and preventive programs, including the targeting of people aged 60 and above;
- •
Implementation of measures aiming at the improvement of earlier diagnosis for all age groups, and for the elderly in particular, such as:
- ∘
Increase awareness of health professionals regarding the possibility of risk situations for HIV and other STDs for people aged 60 years or above
- ∘
Facilitate access to HIV testing, with proper counselling and follow-up
- ∘
Reinforce campaigns encouraging people to know not only their HIV status but also other STDs, such as syphilis and hepatitis
- ∘
- •
Improve the quality of AIDS case report completion by raising awareness among health professional teams.
All authors declare to have no conflict of interest.
