






Dai is a major Chinese ethnic minority group residing in rural areas of the southern part of Yunnan. However, no data exist on the Human Papillomavirus (HPV) prevalence and genotype distribution among Dai women.
MethodA total of 793 participants (Dai=324, Han=251, other ethnic=218) were included in this study. PCR was performed to detect the HPV-positive samples, and genotyping was performed with an HPV Geno-Array.
ResultThe overall HPV prevalence was very low among Dai women compared to the others. The prevalence of high-risk-HPV infections was significantly higher (p=0.001) among other ethnic women (22.0%) than that among Han (13.1%) and Dai women (7.1%). The overall HPV, high-risk-HPV, single and multiple infection prevalence among rural women were 12.9%, 12.1%, 12.3%, and 0.5%, respectively. HPV-16 (5.5%) was shown to be the most prevalent genotype, followed by HPV-52 (2.6%) and HPV-58 (2.4%). Urban women had relatively higher rates of overall HPV (16.0%), high-risk-HPV (14.1%), single genotype (11.9%), and multiple genotype (4.1%) infections. In urban women, HPV-52 (3.6%) was the most prevalent genotype, followed by HPV-39 (2.7%) and HPV-16 (1.2%). In the urban area, HPV prevalence was highest in women aged <29 years, but declined with increasing age. However, in rural women, the highest HPV prevalence was observed among women at older age (>50 years). Education and smoking habit were significantly associated with HPV infection among both rural and urban area women (p<0.001).
ConclusionThe prevalence and genotype distribution of HPV varied among ethnic women in urban and rural area of Yunnan Province.
Human Papillomavirus (HPV) infection is an established cause of cervical cancer, which is a leading cause of death in women of developing regions of the world.1 The People's Republic of China is the homeland of approximately 1.3 billion inhabitants and is the most densely populated country worldwide. In China, there have been 78,400 new cases of cervical cancer reported in 2010,2 causing 20,000 deaths.3
Epidemiologically, the prevalence and genotype distribution of HPV substantially vary with respect to age, ethnicity, developmental level, and health facility.4 Worldwide, the prevalence of HPV is approximately 11–12%, with significant regional variation. The highest HPV prevalence has been reported in Africa (24%), followed by Latin America (16%), and Eastern Europe (21%).5 Significant regional variations in HPV genotype distribution have also been reported. In general, HPV-16 is more frequent in all continents worldwide, whereas the distribution of other genotypes varies from region to region. HPV-18 is the second leading genotype in Europe and South America, whereas HPV-52 and HPV-58 are more dominant in Asia.6
China is the second leading world economy. The National Central for Cancer Registry, which was established in the 1960s, was expanded to cover 31 provinces in 2009; however, it only covers the urban population. Thus, there is a lack of data on disease burden in ethnic populations who reside in mostly remote areas, and the existing cancer-related figures do not represent the whole population.7 Yunnan is a hard, hilly area, with 26 Chinese government state-certified ethnic groups scattered among various concentrated community areas that have completely different norms and traditions. Southern Yunnan bordered with South-east Asian countries and likewise many ethnic groups live on both sides of the border. Most groups such Dai, Hani etc. are certified ethnic groups in China and South-east Asian countries. However, the norms and costumes of these groups vary. As such, the Dai ethnic group, with a population of about 1.2 million, mainly lives in rural areas of the southern part of Yunnan Province particularly in Xishuangbanna prefecture.8 Tibetans are typically settled in highland and mountainous areas, the Naxi group lives in low, hilly areas. The Hani people mainly work in agricultural farming, and live in remote mountainous areas. The Han group represents the ethnic majority, comprising 92% of the total population of China, and they are equally distributed throughout China. They are well educated, mostly belonging to the ruling class, and reside in urban areas. Mass immunization with HPV vaccines has the potential to minimize cervical cancer incidence in women, but the available HPV vaccine only controls the type of HPV for which it is formulated. Furthermore, the vaccine undergoing trials has been formulated based on data recoded from developed areas. Due to the variation in prevalence and genotype distribution of HPV worldwide, and particularly in China, investigating the prevalence and genotype distribution of HPV among various populations of Yunnan Province would be very useful for designing a strategy for HPV control. According to our best knowledge, there are no reports on the prevalence and genotype distribution of HPV among Dai women in comparison with other ethnicity. Therefore, this study was designed to determine the prevalence rate of HPV and its genotype distribution among women of Dai and other ethnicity in southern of Yunnan Province, China and to identify factors associated with HPV infection in rural and urban areas of Yunnan Province.
Materials and methodsStudy population and designA total of 793 (Dai=324, Han=251, other ethnic=218; 381 rural and 412 urban) women were recruited from four different towns and villages of the southern of Yunnan Province, in 2014. To be included in the study the woman should: (1) be mentally and physically normal; (2) be aged 18 years or more; (3) be a permanent resident of local area; (4) not be virgin; (5) not be presently pregnant; (6) have not undergone a total uterine or cervical resection; and (7) be willing to undergo HPV testing and provide consent to participate in the present study. Due to ethnic custom, community meetings were organized in which local community leaders were requested to talk about the importance of this study. The interested women were requested to visit the local community medical (hospital) center, and the object of study was again explained individually.
Questionnaire and descriptionsA standardized questionnaire was especially developed for this study containing the following items:
- -
Demographic data: area (rural or urban), ethnic background, age, education;
- -
Sexual behavior: age at first intercourse, married (polyandry or not) or unmarried, number of lifetime sexual partners, condom use;
- -
Medical and reproductive history: participation in cervical cancer screening, history of sexually transmitted infections, pregnancies, number of babies;
- -
Smoking habits: active or past smoker, regular cigarettes or traditional Chinese tobacco products.
All participants were interviewed by a trained interviewer in the local dialect of Chinese in a separate room using the standardized. After the interview, a qualified gynecologist did the pelvic examination and collected two cervical samples with a cyto-brush (Hybribio) for HPV genotyping and cytological analysis.
DNA extraction and histopathological analysisThe DNA extraction process was completed through the DNA Extraction Kit (Qiagen, Valencia, CA, USA) by following the recommendation of manufacturer.9 The cervical intraepithelial neoplasia grading and cervical cancer was diagnosed according to the World Health Organization classification system (CIN I–III).10
HPV detection and genotypingSamples that tested positive for β-globin were analyzed by PCR amplification of HPV DNA.11 HPV-positive samples were identified by PCR with universal L1 primer MY09/11 and GP5/6 systems.12 DNA from HeLa and Caski cell lines were used as positive controls, and mixtures without sample DNA were used as negative controls. HPV genotypes were determined using an HPV GenoArray Test Kit (Hybribio, Chaozhou, China), according to the manufacturer's instructions. Geno-Array is an L1 consensus primer-based PCR assay13 that is capable of amplifying 23 HPV genotypes, including 13 HR-HPV (high-risk human papillomavirus) genotypes (HPV-16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66 and 68), three PHR-HPV (Potential high-risk human papillomavirus) genotypes (HPV-53, 66, and 81) and seven LR-HPV (low-risk HPV) genotypes (HPV-6, 11, 42, 43, 44, and 61). The assay was conducted according to the manufacturer's recommendations. PCR was performed in a reaction volume of 25μL containing 5μL of DNA template, 19.25μL of the provided master mix, and 0.75μL DNA Taq polymerase, using a Perkin-Elmer GeneAmp PCR System 9700 (Applied Biosystems, USA). The amplification procedure was performed as follows: 9min of denaturation at 95°C, followed by 40 cycles of 20s of denaturation at 95°C, 30s of annealing at 55°C, 30s of elongation at 72°C, and a final extension for 5min at 72°C.
All the samples that were identified as positive through PCR were genotyped with two methods: Geno-Array test and direct sequencing. For the DNA sequencing new PCR was run with a reaction mixture of 50μL containing 6μL of the DNA extract, 1μL of 10μmolar MY09 primer, 1μL of 10μmolar MY11 primer and 25μL of the provided master mixture, and 15μL dH2O. The consensus primer products were separated by electrophoresis on a 2% agarose gel and purified with a Tiangel (TIANGEN Biotech (Beijing) Co., Ltd) PCR purification kit. The DNA was then directly sequenced using the ABI PRISM Big Dye Terminator Cycle Sequencing Ready Reaction (Invitrogen, Beijing, CN) on an ABI 310 DNA analyzer. The nucleotide sequences were aligned and compared with those of known HPV genotypes available through Genbank by using the BLAST 2.0 software server (http://www.ncbi.nih.gov/blast). The sample was identified as a particular HPV genotype if the sequence was 95% homologous with the reference standard.
Statistical analysisThe HPV prevalence rates, including the total rates, and the rates for single- and multiple-genotype infections were compared using the Chi-square test. Corresponding 95% confidence intervals (CIs) were estimated by binomial distribution analysis. The associations between potential risk factor variables with HPV infection in women were assessed by univariate and multivariate logistic regression analyses. Collinearity in the multivariate analysis was evaluated by the tolerance and the goodness-of-fit of the logistic models measured by the Hosmer–Lemeshow test. A p-value less than 0.05 was regarded as statistically significant. The statistical analysis was performed using SPSS version (Chicago, USA) 20.0.
Ethical statementThe study project was in line with the Helsinki Declaration and approved by the Ethics Committee at Kunming University of Science and Technology and the Center for Disease Control and Prevention (CDC) in Yunnan Province, China.
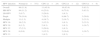
ResultsEthnic differences in the prevalence of HPVThe prevalence of any HPV genotype was higher among other (22.0%) ethnic groups followed by Han (13.9%) and Dai (9.9%) ethnicities, but the difference was not statistically significant (p=0.06). However, HR-HPV prevalence was significantly higher (p=0.015) among other ethnic women (22.0%) compared to Han (13.1%) and Dai (7.1%) women. Single HPV genotype infection was also more frequent among other ethnic women (19.7%) followed by Han (11.1%) and Dai (7.7%) women, but the difference was not significant (p=0.12). Multiple HPV genotype infection prevalence rate among Han (2.8%) women was similar among other ethnic women (2.3%) and Dai women (2.2%) (p=0.83). The HPV genotype distribution among women of the various ethnic groups is shown in Table 1.
The prevalence of HPV and genotype distribution among women of different ethnicities.
| Variables | Dai (n=324) | Others (n=218) | Han (n=251) | p-Valuea | |||
|---|---|---|---|---|---|---|---|
| Positive | P% (95%CI) | Positive | P% (95% CI) | Positive | P% (95% CI) | ||
| Overall | 32 | 9.9 (5.65–13.1) | 48 | 22.0 (16.5–27.5) | 35 | 13.9 (9.4–18.4) | 0.06 |
| High risk | 23 | 7.1 (4.3–9.9) | 48 | 22.0 (16.5–27.5) | 33 | 13.1 (8.9–17.3) | 0.015 |
| Low risk or Mix | 9 | 2.8 (2.7–5.5) | – | 2 | 0.8 | – | |
| Single | 25 | 7.7 (4.8–11.5) | 43 | 19.7 (14.4–25.0) | 28 | 11.1 (7.2–15.0) | 0.12 |
| HPV-16 | 4 | 1.2 | 15 | 6.9 (3.5–10.3) | 7 | 2.8 (0.8–4.8) | 0.2 |
| HPV-52 | 8 | 2.5 (0.8–4.2) | 11 | 5.0 (2.1–7.9) | 6 | 2.4 (0.5–4.3) | 0.94 |
| HPV-39 | 3 | 0.9 | 4 | 1.8 (0.04–3.6) | 6 | 2.4 (0.5–4.3) | 0.16 |
| HPV-58 | 4 | 1.2 | 6 | 2.7 (0.55–4.8) | 2 | 0.8 | 0.75 |
| HPV-68 | 2 | 0.6 | 3 | 1.4 | – | – | – |
| HPV-51 | – | – | 1 | 0.4 | 2 | 0.8 | – |
| HPV-61 | – | – | 1 | 0.4 | 1 | 0.4 | – |
| HPV-66 | 1 | 0.3 | – | 1 | 0.4 | – | |
| HPV-33 | 1 | 0.3 | 1 | 0.4 | – | – | – |
| HPV-81 | 1 | 0.3 | – | – | – | – | – |
| HPV-84 | 1 | 0.3 | – | – | – | – | – |
| HPV-31 | – | – | 1 | 0.4 | – | – | – |
| HPV-11 | – | – | – | – | 1 | 0.4 | – |
| HPV-53 | – | – | – | – | 1 | 0.4 | – |
| HPV-56 | – | – | – | – | 1 | 0.4 | – |
| Multiple | 7 | 2.2 (0.6–3.8) | 5 | 2.3 (0.3–4.3) | 7 | 2.8 (0.8–4.8) | 0.83 |
| Double | 6 | 1.8 (0.4–3.2) | 5 | 2.3 (0.3–4.3) | 7 | 2.8 (0.8–4.8) | 0.45 |
| Triple | 1 | 0.3 | – | – | – | – | – |
n, total number of cases; P%, prevalence percentage; 95% CI, 95% confidence interval were obtained by using binomial distribution analysis model.
HPV DNA was detected in 12.9% of rural women, of whom 12.3% were infected with a single HPV genotype, 0.5% with multiple genotypes, 12.1% with an HR-HPV genotype, and 0.8% was infected with a LR-HPV genotype. Eight different HPV genotypes were identified, among which HPV-16 (5.5%) was the most prevalent, followed by HPV-52 (2.6%) and HPV-58 (2.4%) (Table 1). In urban women, HPV DNA was detected in 66 participants; 49 women were infected with a single HPV genotype and 17 with multiple HPV genotypes. HR-HPV genotype was detected in 14.1% of urban women. A total of 13 HPV genotypes were detected, among which HPV-52 (3.6%) was the most prevalent type, followed by HPV-39 (2.7%), and HPV-16 (1.2%). Some uncommon genotypes such as HPV-61 and HPV-84 were also detected (Table 2).
The prevalence of HPV and genotype distribution among rural and urban women.
| Variables | Total (n=793) | Rural (n=381) | Urban (n=412) | p-Valuea | |||
|---|---|---|---|---|---|---|---|
| Positive | P% (95% CI) | Positive | P% (95% CI) | Positive | P% (95% CI) | ||
| Overall | 115 | 14.5 (12.1–16.9) | 49 | 12.9 (9.5–16.3) | 66 | 16.0 (12.5–19.5) | 0.2 |
| High risk | 104 | 13.1 (11.8–15.5) | 46 | 12.1 (8.8–15.4) | 58 | 14.1 (10.7–14.5) | 0.4 |
| Low risk or Mix | 11 | 1.4 (0.6–2.2) | 3 | 0.8 | 8 | 1.9 | |
| Single infection | 96 | 12.1 (9.8–14.4) | 47 | 12.3 (8.0–15.5) | 49 | 11.9 (8.9–15.0) | 0.5 |
| HPV-16 | 26 | 3.3 (2.1–4.5) | 21 | 5.5 (3.2–7.8) | 5 | 1.2 (0.02–2.2) | 0.001 |
| HPV-52 | 25 | 3.1 (1.9–4.3) | 10 | 2.6 (1.0–4.2) | 15 | 3.6 (1.8–5.4) | 0.5 |
| HPV-39 | 13 | 1.6 | 2 | 0.5 | 11 | 2.7 | 0.01 |
| HPV-58 | 12 | 1.5 | 9 | 2.4 | 3 | 0.7 | |
| HPV-68 | 5 | 0.5 | 1 | 0.3 | 4 | 1.0 | 0.2 |
| HPV-51 | 3 | 0.4 | 3 | 0.7 | |||
| HPV-61 | 2 | 0.2 | 2 | 0.5 | |||
| HPV-66 | 2 | 0.2 | 1 | 0.3 | 1 | 0.2 | |
| HPV-33 | 2 | 0.2 | – | 2 | 0.5 | ||
| HPV-81 | 1 | 0.1 | – | 1 | 0.2 | ||
| HPV-84 | 1 | 0.1 | – | 1 | 0.2 | ||
| HPV-31 | 1 | 0.1 | 1 | 0.3 | |||
| HPV-11 | 1 | 0.1 | – | 1 | 0.2 | ||
| HPV-53 | 1 | 0.1 | – | 1 | 0.2 | ||
| HPV-56 | 1 | 0.1 | – | 1 | 0.2 | ||
| Multiple infection | 19 | 2.4 (1.3–3.5) | 2 | 0.5 | 17 | 4.1 (2.2–6.0) | 0.001 |
| Double infection | 18 | 2.3 (1.3–3.3) | 2 | 0.5 | 16 | 3.9 (2.0–5.8) | |
| Triple infection | 1 | 0.1 | – | 1 | 0.2 | ||
n, total number of cases; P%, prevalence percentage; 95% CI, 95% confidence interval were obtained by using binomial distribution analysis model.
According to the results of HPV analysis, 14.5% of the samples were positive for HPV infection; 12.1% positive for single genotype infections and 2.4% positive for multiple genotype infections. A total of 15 HPV genotypes were reported. HR-HPV genotypes (13.1%) were substantially more common than other genotypes (1.4%). HPV-16 was the most commonly detected genotype (3.3%). The distribution of the other leading genotypes was as follows: HPV-52 (3.1%), HPV-39 (1.6%), and HPV-58 (1.5%) (Table 2).
Abnormal cytology was found in 42 cervical samples: 24 were categorized as CIN1, 12 as CIN2, and the remaining six as CIN3. Overall, 59.5% of these samples (25/42) were positive for HPV. The HPV prevalence was 45.8% (11/24) among CIN1 samples and 83.3% in CIN2 and CIN3 samples. The prevalence of HR-HPV genotypes increased as the infection progressed to advanced lesions (Table 2). HPV-16 was most frequent in advanced abnormal cervical lesions CIN3 followed by HPV-39 and HPV-58. The most frequently detected genotypes in CIN1 and CIN2 lesions were HPV-52 and HPV-58 (Table 3).
HPV prevalence according to histopathological analysis.
| HPV infection | Normal (n=751) | CIN1 (n=24) | CIN2 (n=12) | CIN3 (n=6) |
|---|---|---|---|---|
| Overall | 89 (11.8) | 11 (45.8) | 10 (83.0) | 5 (83.3) |
| HR-HPV | 84 (11.2) | 6 (25.0) | 9 (75.0) | 5 (83.3) |
| LR-HPV | 5 (0.7) | 5 (20.8) | 1 (8.3) | – |
| Single | 78 (10.4) | 7 (29.2) | 8 (66.7) | 3 (50.0) |
| Multiple | 11 (1.5) | 4 (16.7) | 2 (16.7) | 2 (33.3) |
| HPV-16 | 19 (2.5) | 3 (12.5) | 1 (8.3) | 2 (33.3) |
| HPV-39 | 9 (1.2) | 2 (8.3) | 1 (8.3) | 1 (16.7) |
| HPV-52 | 17 (2.3) | 5 (20.8) | 1 (8.3) | – |
| HPV-58 | 6 (0.8) | 3 (12.5) | 2 (16.6) | 1 (16.7) |
| HPV-33 | – | 1 (4.2) | 1 (8.3) | – |
The HPV prevalence among women from rural areas increased from 8.7% in the young age group (<29 years) to 31.7% in the old age group (>50 years) (Table 4). Similar prevalence trends were also observed for HR-HPV and single genotype infections, with little variation. In women from urban areas, the young age group (<29 years) had the highest rates of overall HPV (22.2%), HR-HPV (19.0%), and single genotype (17.5%) HPV infection, while the infection rate declined thereafter with increasing age (Table 3). Education and smoking were found to be significantly associated with HPV infection in both groups of women (p<0.001), whereas drinking habits and number of pregnancies were only associated with acquiring HPV infection in rural women (p<0.001, Table 4). However, the other potential risk factors such as occupation, age at first intercourse, condom use, number of sexual partners, married (polyandry or not) or unmarried, history of sexually transmitted infections and past history of Pap smear test that were analyzed in this study appeared to have no influence on HPV infection in either group (Table 5).
Comparison of age-specific overall, high-risk, single, and multiple HPV infection prevalence in four age-groups among rural and urban women.
| Rural women | |||||
|---|---|---|---|---|---|
| HPV infection | <29 (n=80) | 30–39 (n=115) | 40–49 (n=145) | >50 (n=41) | p-Value |
| Overall | 7 (8.7) | 13 (11.3) | 16 (11.0) | 13 (31.7) | 0.008 |
| HR-HPV | 7 (8.7) | 13 (11.3) | 14 (9.6) | 12 (29.3) | 0.02 |
| LR-HPV | – | – | 2 (1.4) | 1 (2.4) | |
| Single | 7 (8.7) | 13 (11.3) | 15 (10.3) | 12 (29.3) | 0.02 |
| Multiple | 1 (0.7) | 1 (2.4) | |||
| Urban women | |||||
|---|---|---|---|---|---|
| HPV infection | <29 (n=63) | 30–39 (n=153) | 40–49 (n=129) | >50 (n=67) | p-Value |
| Overall | 14 (22.2) | 26 (17.0) | 21 (16.3) | 5 (7.5) | 0.03 |
| HR-HPV | 12 (19.0) | 26 (17.0) | 16 (12.4) | 4 (6.0) | 0.01 |
| LR-HPV | 2 (3.2) | – | 5 (3.9) | 1 (1.5) | |
| Single | 11 (17.5) | 20 (13.1) | 15 (11.6) | 3 (4.5) | 0.02 |
| Multiple | 3 (4.8) | 5 (3.3) | 7 (5.4) | 2 (3.0) | 0.9 |
Detection of cervical human papillomavirus (HPV) DNA according to potential risk factors in rural and urban women.
| Variable | Rural (n=381) | Urban (n=412) | ||||||
|---|---|---|---|---|---|---|---|---|
| Total cases | Positives | ORa (95%CI) | p-Value | Total cases | Positives | OR2 (95% CI) | p-Valueb | |
| Pregnancy | 0.012 | 0.16 | ||||||
| Single | 113 | 13 | 1 | 299 | 37 | 1 | ||
| Double | 176 | 19 | 0.22 (0.08–0.62) | 78 | 20 | 2.1 (0.9–4.5) | ||
| Multiple | 92 | 17 | 0.48 (0.18–1.29) | 35 | 9 | 2.1 (0.7–6.8) | ||
| Active smoker | 0.002 | 0.03 | ||||||
| Yes | 241 | 26 | 1 | 367 | 64 | 1 | ||
| No | 140 | 23 | 3.9 (1.7–9.5) | 45 | 2 | 5.5 (1.8–17.4) | ||
| Drinking | 0.021 | 0.15 | ||||||
| Yes | 225 | 13 | 1 | 74 | 23 | 1 | ||
| No | 156 | 36 | 2.45 (1.1–5.3) | 338 | 43 | 0.3 (0.06–1.54) | ||
| Education | 0.009 | 0.001 | ||||||
| Graduate | 17 | 0 | – | 178 | 29 | 1 | ||
| High | 15 | 0 | – | 66 | 12 | 0.9 (0.4–2.1) | ||
| Middle | 75 | 8 | – | 84 | 6 | 0.1 (0.02–0.36) | ||
| Primary | 188 | 19 | – | 47 | 15 | 0.3 (0.08–1.2) | ||
| No | 86 | 22 | – | 37 | 4 | 0.1 (0.01–0.4) | ||
| Employment | 0.5 | 0.56 | ||||||
| No work | 24 | 2 | 1 | 76 | 8 | 1 | ||
| Business | 353 | 47 | 0.4 (0.07–2.1) | 121 | 31 | 0.7 (0.3–1.9) | ||
| Job | 4 | – | – | 215 | 27 | 1.3 (0.4–3.9) | ||
n, total number of participants.
Vaccination against HPV is a possible long-term solution for eradicating cervical cancer in developing countries, particularly in China, where HPV-related infection is a leading cause of morbidity (12%) and mortality (14%).14 In China, a prophylactic HPV vaccine is undergoing a phase III trial.15 Furthermore, the available HPV vaccine is genotype specific and only protects against infections by HPV of the genotype for which it is formulated. To maximize the effectiveness of HPV vaccination in China, determining the variation of HPV prevalence and genotype distribution among the various ethnicities in different geographical regions of the country is essential. In the current study, 14.5% (Table 2) of the participants were positive for HPV infection. Compared to similar studies conducted in Yunnan province, this prevalence rate is similar to that reported in a study conducted in Southern of Yunnan province (14.7%), China.16 However, the frequency of infections with oncogenic HPV genotypes (13.1%) was slightly higher than that found in a population-based study conducted in Shanxi, China (12.2%)17 and that found in South Vietnam (10.9%).18
In China, HPV prevalence and its genotype distribution have previously been described among Naxi women (11.9%), Tibetan women (27.4%),19 Uyghur women (7.3%), and Han women (6.7–29.6%).17,20 The overall HPV prevalence in other ethnic women (22.0%) (Table 1) in this study was very high as compared with rate reported among Naxi (11.9%), but lower than that of Tibitan (27.4%) in north-western Yunnan. The HPV prevalence measured among Han women (13.9%) was higher than that reported among Han in southern of Yunnan (12.6),21 and the prevalence of HPV among Dai women (9.9%) was lower than the worldwide infection rate (11–12%)22 and the prevalence reported from other regions of China and Korea.6 In southern of Yunnan, living and social rules vary among ethnic groups. The majority of individuals in the other ethnic population are illiterate, have a high fertility rate, mainly work in agricultural farming, and live in remote mountainous areas with poor sanitary conditions. In contrast, the majority of Dai individuals are educated with religious education, live in very clean, well-lighted and well-ventilated constructed double stories bamboo house in which downstairs are used for livestock and upstairs are used by people. Among Dai people, endogamy is common, while among Han or other ethnic group it is forbidden. Similarly, marriage between relatives is common among Dai while among other ethnic group such as Han, Hani, and Zhuang it is strictly forbidden. Similarly, among some ethnic groups, such as Tibitan and Hani, polyandry is common, while among Dai it is strictly forbidden. We suggest that social backgrounds and cultural traits might be responsible for the high HPV infection rate among other ethnic women in this region because the Dai and other ethnic women live in same area but under different sanitary conditions.
Our population-based study compared the HPV prevalence among women living in rural and urban areas of Yunnan Province. Our study showed that some rural populations in China have a lower HPV prevalence (12.9%) than that of urban populations (16.0%). However, these findings are in contrast to those of many studies from China, in which the HPV prevalence among rural populations was higher than that among urban populations.15,17 The HPV prevalence rate among rural populations was comparable to the data reported from other regions of China, such as Henan Province (12.3–13.0%).23 In the current study, the prevalence among urban women (16.0%) was comparable to the results reported from various parts of China.24 A large difference in the HR-HPV prevalence was found between rural women (12.1%) and urban women (14.1%). Compared with similar studies from China, the HR-HPV prevalence (11.9%) in rural areas of southern of Yunnan Province16 was similar than that reported in this study (12.1%), whereas the HPV prevalence among urban women was higher than that reported for Beijing (9.9%),25 but lower than that reported in a pooled analysis (17.7%) by Zhao et al.26 The most striking feature in the epidemiology of HPV infections among both populations is the high frequency of multiple-genotype infections among urban women (4.1%) compared with rural women (0.5%). The relatively higher frequency of multiple-genotype infections in urban women is consistent with data from Qujing City of Yunnan Province.27 The higher prevalence of overall HPV, oncogenic HPV, and multiple-genotype HPV infections in urban women might partly be due to lifestyle and standards of living. Furthermore, the difference cannot be due to technical reasons because both groups were randomly selected, the cervical samples were collected by the same qualified gynecologist, and all of the samples were analyzed under the same roof using the same chemicals.
A total 15 genotypes were identified among both populations. However, the HPV genotype distribution was diverse among both groups. HPV-16 was recognized to be the most prevalent genotype, followed by HPV-52 and HPV-58, in rural populations. These observations are in complete agreement with the study conducted in Shanxi, Lijiang Yunnan province China, in which a relatively high percentage of HPV-16 and then of HPV58 infection was observed16,28 confirming the importance of HPV-58 and HPV-52 infection in Asia,32 particularly in China. HPV-52 (3.6%) was more prevalent among urban women, followed by HPV-39 (2.7%) and HPV-16 (1.2%). The variation in genotype prevalence may be due to the geographic location of the participants and the biological interactions among genotypes and patients’ immune status.6,29 Another possible interpretation may involve variation in the genotyping technique. However, this is not a convincing interpretation because many previous studies reported that HPV-52 and HPV-58, not HPV-16, were the leading HPV genotypes in Asia and particularly in China. Interestingly, another oncogenic type, HPV-68 (1.0%), was also common in this population, despite being previously considered an uncommon genotype.6
The age-specific prevalence curve for rural participants was relatively similar to the findings of studies conducted in Shenyang City, Shanxi Province.17 The HPV prevalence was directly correlated with age, with the highest prevalence observed among older age groups. The prevalence of HPV in rural women increased with age and peaked in the older age group (>50 years), a trend that may be caused by a weakened immune system in the infected population. This pattern is in agreement with previous studies conducted in high-resource countries,30,31 China,17 and India.32 In addition to the overall prevalence of HPV, the age-specific prevalence in urban women also differed from that of rural women. Younger women had the highest infection rates, and the prevalence decreased with increasing age. These findings are in line with data reported in previous studies19,29 suggesting that younger women have higher exposure to HPV infection than older women. However, these findings differed from those for various part of China, where the HPV prevalence was similar in all age groups.17 The flat age curve in the rural population indicates that in many populations in the developing world, women are not exposed to HPV at a young age.17 As most women in rural areas are married and have single sexual partner, the less pronounced second peak of HPV infection in middle age might be due to husbands’ extramarital sexual relationships. This risk factor has already been verified in a pooled analysis conducted by the International Agency for Research on Cancer (IARC).33 The high HPV prevalence among the older age group of rural women might be attributable to weak immune responses for clearing infection or to a high incidence of HPV infection. Nulliparous women were at lower risk for acquiring HPV infection than multiparous women.33 In this study, we also found a clear trend toward an increasing risk of HPV infection with increasing parity among women from both areas. However, women with two or more babies in the rural areas only were at a significantly higher risk of being infected with HPV. The results of previous reports regarding the role of smoking in the acquisition of HPV infection are controversial.33,34 In the present study, education and drinking were significantly associated with HPV infection in both groups, and smoking was only linked with acquisition of HPV infection in rural women.35 Based on these findings, we suggest that there must be a correlation between smoking and another risk factor such as ethnicity, age of sex, drinking habit, contraceptive use, and sexual behaviors. We will attempt to explain the correlations of potential risk factors in our future study.
ConclusionTo the best of our knowledge, this is the first Dai ethnic population-based study conducted in Yunnan, China. Significantly higher prevalence rates of HR-HPV were found among the other ethnic women compared with the Dai and Han women. Furthermore, a significantly higher prevalence of HPV-16 and HPV-39 were found among urban women as compared to rural women. The results generated from the current report emphasize the requirement of more detailed research to understand the regional differences in the prevalence and genotype distribution of HPV among the various populations. Our study findings also highlight the importance of introducing a next-generation (HPV-52, 58, 39, 68 & 33) HPV vaccine.
Authors’ contributionsZulqarnqin Baloch, Li Yuanyue Xiaomai Wu designed the study, was involved in data collection and genotyping, analyzed the results and wrote the paper. Ma Ke was involved in data collection. Nafeesa Yasmeen helped in data analysis and manuscript writing. Prof. Xueshan Xia and Shi-hua Yang supervised the study. All of the authors read and approved the final manuscript.
Conflicts of interestThe authors declare no conflicts of interest.
We sincerely thank all the participants who took part in this study. This work was financially supported by a research grant from Science and Technology Agency of Yunnan Province, China (2014FB090). The funders played no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
