




This article aims to review the use of antifungal prophylaxis with intravenous fluconazole in premature newborns and the occurrence of Invasive Candidiasis.
MethodsThis is a systematic review with search at databases: PubMed, Capes Portal, Virtual Health Library (BVS – Biblioteca Virtual em Saúde)/Lilacs, Scopus and Cochrane. The keywords used were: “Antifungal”, “Candida” “Fluconazole prophylaxis” and “Preterm infants”.
ResultsInvasive Candidiasis was evaluated in all the twelve items. In eleven of them, there was a statistically significant difference between the groups receiving prophylactic fluconazole, with lower frequency of Invasive Candidiasis, compared to placebo or no prophylaxis group. Colonization by Candida species was also evaluated in five studies; four of them presented statistically lower proportion of colonization in patients with Fluconazole prophylaxis, compared to placebo or no drugs. In one study, there was a significant difference, favoring the use of fluconazole, and reduction of death.
ConclusionStudies indicate the effectiveness of prophylaxis with fluconazole, with reduction in the incidence of colonization and invasive fungal disease. The benefits of prophylaxis should be evaluated considering the incidence of candidiasis in the unit, the mortality associated with candidiasis, the safety and toxicity of short and long-term medication, and the potential for development of resistant pathogens.
The incidence of invasive fungal infection ranges from 2% to 4% in infants with very low birth weight (VLBW<1500g)1 and may affect 4% to 16% of extreme-low birth weight newborns (EBPN<1000g).2–4 Candida species have a higher incidence of invasive candidiasis (IC) in newborns and it is one of the most important causes of morbidity and mortality in the neonatal population.5,6
The immaturity of the immune system and the use of invasive devices, such as mechanical ventilation and central venous catheter, are considered important risk factors for IC.7–9 Prior colonization by Candida sp., delivery route, and cross transmission by the hands of health professionals are also considered predisposing factors. Exposure to broad-spectrum antimicrobial drugs favors the selection of microbiome and the use of post-natal steroids and H2 inhibitors is a factor that favors translocation in the colonized patient to invasive infection.5,8,9
Besides bloodstream infection (Candidemia) Candida may affect other organs, especially heart, urinary tract, retina, and central nervous system (CNS).9 CNS involvement may occur in around 50% of newborns with IC,10,11 and impaired neurological development after infection affects up to 60% of survivors.12 The mortality rate reported in some studies is around 20%,11,13 but it can reach up to 40%.14
Despite evidences and recommendations favoring the use of intravenous fluconazole for prevention of invasive fungal infections (IFI) in neonates,15–17 universal use of antifungal prophylaxis is controversial in the literature. Currently, it is recommended in Neonatal Intensive Care Units (NICU) with fungal infections rates higher than 5%.18,19
Thus, this study aimed to conduct a systematic review on the use of antifungal prophylaxis with intravenous fluconazole in premature newborns and the occurrence of IC (Fig. 1).
Methods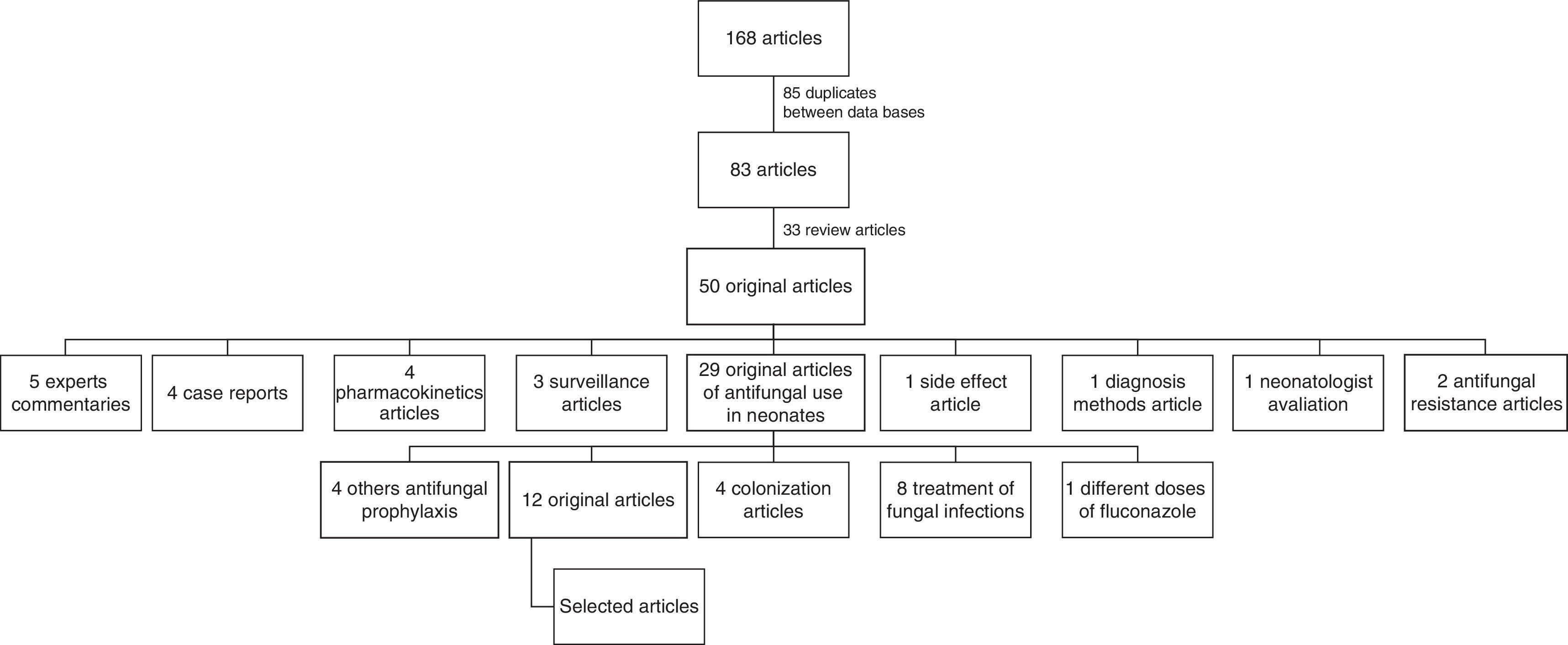
This was a systematic review which included virtual libraries: PubMed, EmBase, Portal Capes, Virtual Health Library (BVS – Biblioteca Virtual em Saúde)/Lilacs, Scopus, and Cochrane databases, without language restriction, with publications until February 2016 without previous date limit considering the first study was in 2001. It also included forward citation tracking. The keywords were “Antifungal”, “Candida”, “Fluconazole prophylaxis” and “Preterm infants” or “very low birth weight”. The search was performed in duplicate by two researchers.
PICO strategy20 was performed considering: Population (P) – infants with birth weight lower than 1500g; Intervention (I): use of antifungal prophylaxis with fluconazole; Comparison (C): no antifungal prophylaxis or use of placebo; Outcome (O): occurrence of Invasive Candidiasis; Study type (S): comparative studies of case–control, cohort, or clinical trials.
A total of 168 articles were found: 54 PubMed articles, 52 Portal Capes articles, 31 BVS articles, 20 Scopus articles, 10 Cochrane articles, and a comparative study obtained in references cited in review articles. Of them, 85 were duplicates among the databases and 83 were chosen for the first selection.
Seventy one studies were excluded. Of them, 33 were reviews and five were experts’ commentaries on articles published in journals indexed in the databases. Eight studies addressed the treatment of fungal infections, two included treatment of resistant Candida species and one was about diagnostic methods. Four were studies on the prevalence of fungal colonization in neonates and other four reports of infection by other fungal species. Three publications focused on epidemiological surveillance studies of invasive fungal infections. Four other studies evaluated prophylaxis of IC with a different antifungal and four addressed a pharmacokinetic evaluation of antifungal agents. In addition, one article examined the occurrence of side-effects with the use of Fluconazole. Furthermore, one article evaluated the adhesion of neonatologists to prophylactic fluconazole use protocol in NICU and one compared different doses of fluconazole.
Twelve studies were eligible for comparative and qualitative analysis, including four randomized clinical trials (RCT), five comparative studies, two case–control studies, and one cohort study.
ResultsWe selected 12 original articles which referred to the prophylaxis of IFI with intravenous use of fluconazole in premature infants, eight observational studies (comparative, cohort and case–control), and four clinical trials published between 2001 and 2014 that evaluated 11,405 newborns, from whom 7416 received prophylactic fluconazole and 3989 received placebo or no prophylactic drugs. The studies varied in birth weight (BW) and inclusion criteria ranged from 750g to 1550g.
Table 1 shows the summary of the articles, considering year of publication, study population, type of intervention, and occurrence of the event of interest (IC).
Original articles selected for systematic review of use of prophylactic Fluconazole in newborns.
| Author | Year | Study | Population | Outcome | p value | Effect | Evidence |
|---|---|---|---|---|---|---|---|
| Kaufman D et al.29 | 2001 | Clinical trial randomized, blinded, placebo controlled | 50 NB<1000g in placebo group 50 NB<1000g in Fluconazol group | Colonization IC Mortality | p<0.001 p=0.008 p=0.22 | Difference in risk 0.18 (95% CI 0.15–0.22) 0.20 (95% CI 0.04–0.36) – | A-I |
| Uko Set al.21 | 2006 | Observational, comparative study, pre and post exposure | 206 NB<1500g no prophylaxis 178 NB<1500g – prophylaxis | CI (after 3o day) Mortality | p=0.07 p=0.644 | OR – 0.166 (95% CI: 0.033–0.709) OR: 0.795; (95% CI: 0.301–2.102) | A-II |
| Manzoni P et al.22 | 2006 | Retrospective comparative study pre and post exposure | 240 NB<1500g – no prophylaxis 225 NB<1500g prophylaxis | IC Colonization Mortality | p<0.0001 p=<0.001 p=0.44 | RR – 0.233 (95% CI 0.113–0.477) RR – 0.406 (95% CI 0.273–0.605) – | A-II |
| Manzoni P et al.32 | 2007 | Clinical trial randomized, blinded, placebo controlled | 106 NB<1500g in placebo group 112 NB<1500g in Fluconazol 6mg/kg group 104 NB<1500g in Fluconazol 3mg/kg group | Colonization Placebo×Fluconazol (3 and 6mg/kg) IC Placebo×Fluconazol (3 and 6mg/kg) Overall mortality | p<0.001 p=0.001 p=1 | RR – 0.30 (95% CI 0.18–0.51) RR=0.25 (95% CI 0.10–0.59) RR=0.88 (95% CI 0.10–0.59) | A-I |
| Parikh TB et al.30 | 2007 | Clinical trial randomized, blinded, placebo controlled | 60 NB<1500g in placebo group 60 NB<1500g in prophylaxis group | Colonization IC Mortality | p=0.003 p=0.835 p=1 | 30 (50%) in placebo group and 11 (19%) in fluconazole group 15 (25%) in placebo group and 16(26.7%) in fluconazole group 17 in placebo group 17 in fluconazole group | B-I |
| Weitkamp J-H et al.23 | 2008 | Comparative study, pre and post exposure | 44 NB<750g or<26 GA – no prophylaxis 42 NB<750g or<26 weeks of GA in Prophylaxis | IC | p=0.004 | 9 cases in 44 infants (20%) No cases in 42 infants | B-II |
| Healy CM et al.24 | 2008 | Comparative study, pre and post exposure | 3012 NB – no prophylaxis 6393 NB: 47 NB≥1.000g+262 NB<1000g in prophylaxis (2002–2006) | CI IC associated Mortality Overall mortality | p=0.05 p=0.004 p=0.13 | 19 IC in pre prophylaxis group (0.6%) and 22 IC in pos-prophylaxis group (0.3%) 4 (21%) in pre prophylaxis group and none in pos prophylaxis group 19% (40 of 206 NB) to 15% (65 of 448 NB) | B-II |
| Rueda K et al.25 | 2010 | Comparative study, pre and post exposure | 271 NB<1250g – no prophylaxis 252 RN<1250g in prophylaxis | IC Overall Mortality IC associated Mortality | p=0.001 p<0.05 p>0.05 | OR=0.13 (95% CI 0.03–0.47) 6%×1% 76%×67% | A-II |
| Rolnitsky A et al.27 | 2012 | Retrospective cohort with historical controls | 130 RN<1000g, or risk factors – Fluconazol prophylaxis 319 historical controls with no prophylaxis | IC | p=0.016 | OR=0.05 (95% CI 0.005–0.52) | A-II |
| Benjamin Jr DK et al.31 | 2014 | Multicentric clinical trial randomized, blinded, placebo controlled | 188 RN<750g in Fluconazol prophylaxis 173 RN<750g in placebo | IC<49 days IC before discharge Mortality<49 days Mortality before discharge Neurodevelopmental impairment | p=0.02 p=0.02 p=0.98 p=0.84 p=0.60 | Difference −6 (CI 95% −11 to −1) Difference −7 (CI 95% −12 to −1) Difference 0 (CI 95% −7 to −7) Difference −1 (CI 95% −9 to 7) Difference 4 (CI 95% −10 to 17) | A-I |
| Cetinkaya M et al.28 | 2014 | Cohort – pre-post intervention | Prophylaxis: 90 NB<1.000g No prophylaxis: 107 NB<1.000g | IC | p=0.03 | Prophylaxis: none IC Control: 5 (4.7%) IC | A-II |
| Kaufman D et al.26 | 2014 | Multicenter case–control | Casos 127 RN<1250g receberam fluconazol Controls; 399 RN<1250g sem profilaxia | IC Candida Bloodstream Infection | p=0.006 p=0.02 | 1 (0.8%) of 127 NB 29 (7.3%) of 399 NB 1 (0.8%) of 127 NB 22 (5.5%) of 399 NB | A-II |
NB, newborn; GA, gestational age; IC, invasive candidiasis; RR, relative risk; OR, odds ratio; 95% CI, 95% confidence interval.
Five studies were only described as comparative, considering pre- and post-exposure periods.21–25 Studies defined as case–control and cohort26–28 were based on historical controls, comparing neonates who were admitted to the NICU in periods before and after implementation of prophylaxis with fluconazole for IC.
Of four clinical trials, three used a fixed dose of fluconazole with a placebo group29–31 and one evaluated two distinct doses of Fluconazole (6mg/kg and 3mg/kg) compared to placebo.32
The event IC was examined in all the 12 studies. In 11 of them, there was a statistically significant difference, with lower rates in groups receiving prophylactic fluconazole for IC, compared to placebo or no drug groups. The randomized, double-blind placebo-controlled study conducted by Parikh et al., 2007,30 found no difference between the incidence of IC between intervention and placebo groups.
The outcome colonization by Candida species in several body sites (skin, nasopharynx, periumbilical region, perineum, gastric aspirate, endotracheal secretion) was evaluated in five studies. Three randomized clinical trials29,30,32 and a comparative study22 found a statistically significant difference between colonization in at least one site searched among the groups, with lower incidence of Candida colonization in the Fluconazole group.
Overall mortality and mortality associated to IC were assessed as an endpoint in six studies: four comparative studies with pre-prophylaxis period and fluconazole prophylaxis period,21,22,24,25 and two trials comparing Fluconazole to placebo.29,31 In only one these studies,24 there was a significant reduction in deaths associated to IC, with 21% mortality in the pre-prophylaxis group versus no deaths in the post-prophylaxis group. Only one clinical trial31 conducted by Benjamin et al. evaluated neurodevelopment at 18–22 months of age in the infants who were randomized to use prophylactic fluconazole or placebo. The authors concluded that the use of Fluconazole did not impair the neurodevelopment of these neonates.
DiscussionThe incidence of IC in different studies and literature reports varies widely ranging between 2 and 4% in neonates with birth weight lower than 1500g (VLBW) to 10–16% in those below 1000g (ELBW).1,2,33 However, some studies showed higher incidences of IC: two studies included VLBW newborns and found an incidence rate of 13.2%32 and 16.7%22 before the prophylactic intervention with fluconazole. Two other studies with ELBW (<1000g) newborns showed an incidence around 20% of IC in groups without prophylaxis.23,29
Two trials were performed at a single center and the number of neonates randomized in each group was small, with 50 or 60 neonates allocated in each group.29,30 But there was no significant difference in baseline characteristics of the groups, and this did not cause selection bias in the statistical analysis.
Some studies did not show effect measures in their results, not describing relative risks, odds ratio or confidence interval between intervention and placebo or control groups.23,24,26,28,30 However, four of them presented statistical significance in reducing IC.
The studies have limitations that should be taken into account when evaluating and generalizing their results. However, the high incidence of complications associated with IC in premature infants, including neurodevelopmental impairment, supports the importance of preventive measures, including the use of prophylactic fluconazole.16
Another study not included in this review evaluated different intervals of fluconazole doses. Kaufman et al.34 evaluated 3mg/kg of fluconazole administered daily or twice a week. The author found no difference in the incidence of IFD between daily and twice a week dose groups.
The Infectious Diseases Society of America (IDSA)35 states that prophylaxis for IC with fluconazole can be considered to VLBW newborns in NICU with rates of candidiasis higher than 10% (AI), based on placebo controlled randomized trials.29,32 It is also recommended that resistance to antifungal agents, toxicity associated to fluconazole, and assessments of neurological development of newborns should be observed (A-III), since there are no studies that have adequately assessed the effects of long-term use of prophylactic fluconazole. Authors do not specify how long such monitoring should be.19,35
In Europe, the Spanish Society of Pediatric Infectious Diseases recommends the use of prophylactic fluconazole at a dose of 3mg/kg, twice a week, throughout the period of risk in preterm infants of VLBW in NICU with incidence of IC greater than 10%,17 based on randomized clinical trials32 and recommendations of Concise Reviews of Pediatric Infectious Diseases.36
Subsequently, the European Society of Clinical Microbiology Infectious Diseases15 recommended antifungal prophylaxis in neonates as AI evidence, considering risk stratification strategy: (a) in NICU with high frequency IC (>5%), fluconazole 3–6mg/kg twice a week, intravenous or orally, is indicated to all infants with birth weight lower than 1000g, based on six systematic reviews and meta-analyses;37–43 (b) in NICU with incidence rate lower than 2%, the decision to use prophylaxis with fluconazole should be made individually (e.g. infants<1000g, with risk factors for IC as central venous catheter, use of third-generation cephalosporins and carbapenems) as evidence B-II.
Although none of the studies examined in this review has been carried out in Latin America, the recommendations of Latin America Invasive Mycosis Network,16 published in 2013, indicate prophylaxis with fluconazole 3mg/kg, twice a week, for six weeks, in neonates of ELBW (<1000g) who are in NICU with high incidence of IC (greater than or equal to 5%). When the incidence is lower than 5%, the use of prophylactic fluconazole may be considered, according to the risk factors of each newborn.
ConclusionThe studies included in this review present the effectiveness of prophylaxis of IC with fluconazole, with significant reduction in the incidence of colonization by Candida species and IC. The potential benefits of antifungal prophylaxis should be evaluated considering cost-effectiveness, efficacy of prophylaxis, and incidence of candidiasis and mortality associated with candidiasis at the NICU. Safety and toxicity of the drug at short and long-term and the potential for development of resistant pathogens should also be taken into account.
FundingUniversidade Federal de Minas Gerais (UFMG)/Fundação de Amparo à Pesquisa do Estado de Minas Gerais (FAPEMIG), Hospital Sofia Feldman – Belo Horizonte/MG – Brasil.
Conflicts of interestThe authors declare no conflicts of interest.
