


Worldwide about 30% of HIV-infected patients are coinfected with HCV or HBV. The HIV/HCV coinfection is more common in individuals who have a history of drug addiction. The aims of this study were to assess the HCV and HBV prevalence in HIV-infected patients and analyze their characteristics.
MethodsWe considered the new HIV diagnoses notified by the regional surveillance system of Tuscany from 2009 to 2013. Descriptive analyses were conducted on the socio-demographic characteristics, routes of transmission, and reason to perform the test. In coinfected patients we assessed the risk for being late presenter (LP) or the risk of having AIDS.
ResultsIn 5 years of surveillance a total of 1354 new HIV diagnoses were notified: 1188 (87.7%) were HIV alone, 106 (7.8%) HIV/HCV, 56 (4.1%) HIV/HBV, and 4 (0.33%) HIV/HCV/HBV. The main risk factor was injection drug use in 52.8% of HCV/HIV cases, while in HIV/HBV patients the main risk factor was sexual exposure. HIV/HBV coinfected patients showed worse clinical and immunological features than HIV and HIV/HCV patients: 78.6% had CD4 count less than 350mm−3 (vs. 54.6% and 62.1%, respectively) and 39.4% had AIDS (vs 20.7% and 7.6%). The risk for being LP triples for HIV/HBV (OR 2.98; 95% IC: 1.56–5.70) than patients with HIV alone.
ConclusionsWe have observed less advanced disease in HIV and HCV-HIV patients compared with HBV–HIV coinfected patients. Moreover, our results show a higher prevalence of HIV/HCV among drug addicts and in the age-group 35–59, corresponding to those born in years considered most at risk for addiction. This study also confirms the finding of a less advanced HIV disease in HIV/HCV coinfected patients.
The Acquired Immune Deficiency Syndrome (AIDS), reported for the first time in literature in 1981, represents the final clinical stage of infection by the human immunodeficiency virus (HIV).1
The advent of Highly Active Anti-Retroviral Therapy (HAART) has changed the natural history and epidemiology of HIV infection. In particular, the mortality rate has decreased as a consequence of the reduction in the number of people who develop the condition of AIDS. In 2012, people living with HIV infection or AIDS were 35 million worldwide, while the new diagnoses were about 2.3 million, with a decrease of 33% compared to 2001, when new infections were approximately 3.4 million.2
Sub-Saharan Africa is the most affected region. Recently, 1 million new diagnoses were reported. South and South-East Asia reported 270 thousand new diagnoses. In Europe, HIV infection remains a problem of major public health importance. Italy, in 2012, reported 3853 new diagnoses of HIV infection and 715 cases of AIDS, amounting to an incidence rate of 6.5 and 1.7 cases per 100,000 inhabitants, respectively. These rates, although lower than the European average, are higher than the average of other European Union and European Economic Area (EU/EEA) countries.3
Worldwide, about 1 million deaths per year are attributed to hepatitis B or C viral infections (HBV or HCV). This represents 2.7% of all cause mortality. The most common causes include hepatocellular carcinoma. Moreover, 57% of cases of liver cirrhosis and 78% of liver cancer are caused by HBV and HCV.4 HBV, HCV, and HIV share the same transmission routes. It has been estimated that worldwide about 30% of people with HIV are coinfected with HCV or HBV.5 Usually, the HIV/HCV co-infection is more common in individuals who have a history of drug addiction.6 Several studies have also demonstrated that such coinfections present a major risk for liver fibrosis progression and subsequent evolution to cirrhosis.7
Based on these premises, the objectives of this study were to evaluate the prevalence of HIV/HCV and HIV/HBV coinfections in Tuscany and to analyze their characteristics.
MethodsIn Italy, AIDS was declared a nationally notifiable infectious disease by Ministerial Decree No. 288 of November 28, 1986 and was subsequently subjected to special notification by filling in a special form. In 2008, new diagnoses of HIV infections were also subjected to mandatory notification.
In Tuscany, the management of the HIV regional surveillance system has been improved since 2009 and requiring notification of new HIV diagnoses.
In this study, we considered the cases of new HIV diagnoses notified in Tuscany from 2009 to 2013 to the Regional Surveillance System. This dataset contained information about patient gender, age, nationality, mode of transmission, reason for being tested, CD4 lymphocytes count, HIV viral load, and AIDS diagnosis. We analyzed the prevalence of coinfection with HBV (based on the presence of antigen surface – HBsAg), HCV (based on the presence of anti-HCV antibody, which identifies people who have been infected with the virus), or both. We considered the following clinical and immunological conditions: (1) late presentation (LP): persons presenting for care with a CD4 count below 350cells/μL or with an AIDS-defining event (such as bacterial infections, candidiasis, cryptococcosis, cytomegalovirus retinitis, Kaposi sarcoma, lymphoma), irrespective of CD4 cell count; (2) presentation with advanced HIV disease (AHD): persons presenting for care with a CD4 count below 200cells/μL or with an AIDS-defining event, regardless of the CD4 cell count8; and (3) AIDS condition, defined as having HIV and an opportunistic infection, regardless of the CD4 cell count.
Socio-demographic characteristics, risk factors, reasons for being HIV tested, and the clinical and immunological features of patients were analyzed in the following four groups of patients: HIV monoinfection, HIV/HBV, HIV/HCV, and HIV/HBV/HCV infected patients. A chi-square test was performed to analyze the association between each variable and the condition of coinfection.
Multivariate logistic regression analysis was used to explore if the coinfection conditions were associated with LP, AHD or AIDS, adjusting for gender, age, nationality, and risk factors.
Statistical analyses were performed using STATA SE 12.0 statistical software.
ResultsIn five years of surveillance (2009–2013), 1402 new HIV diagnoses were notified in Tuscany, with an incidence rate of 7.6 per 100,000 residents. Information on HBV or HCV coinfection was available for 1354 (96.6% of the total number of the new HIV diagnoses) HIV infected patients: 1188 (87.7%) were monoinfected, 106 (7.8%) were coinfected with HIV/HCV, 56 (4.1%) with HIV/HBV, and 4 (0.3%) with HIV/HCV/HBV.
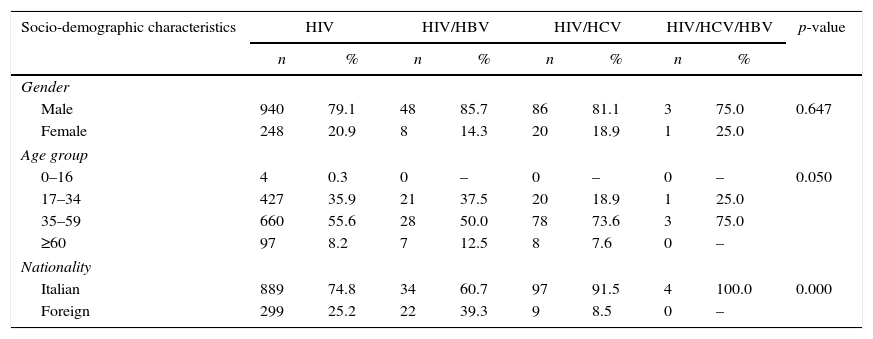
In the HIV monoinfected, HIV/HBV, and HIV/HCV groups 20.9%, 14.3%, and 18.9% were female, respectively (Table 1). Italian nationality was significantly different in three groups of patients: 91.5% of HIV/HCV patients, 60.7% of HIV/HBV, and 74.8% of HIV monoinfection. Most (73.6%) of the HIV/HCV patients were diagnosed in the 35–59 age group (median age 43), compared to 50.0% of HIV/HBV patients (median age 38) and 55.6% of HIV monoinfected patients (median age 39).
Socio-demographic characteristics of HIV, HIV/HBV, HIV/HCV, HIV/HCV/HBV patients notified in Tuscany (2009–2013).
| Socio-demographic characteristics | HIV | HIV/HBV | HIV/HCV | HIV/HCV/HBV | p-value | ||||
|---|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | ||
| Gender | |||||||||
| Male | 940 | 79.1 | 48 | 85.7 | 86 | 81.1 | 3 | 75.0 | 0.647 |
| Female | 248 | 20.9 | 8 | 14.3 | 20 | 18.9 | 1 | 25.0 | |
| Age group | |||||||||
| 0–16 | 4 | 0.3 | 0 | – | 0 | – | 0 | – | 0.050 |
| 17–34 | 427 | 35.9 | 21 | 37.5 | 20 | 18.9 | 1 | 25.0 | |
| 35–59 | 660 | 55.6 | 28 | 50.0 | 78 | 73.6 | 3 | 75.0 | |
| ≥60 | 97 | 8.2 | 7 | 12.5 | 8 | 7.6 | 0 | – | |
| Nationality | |||||||||
| Italian | 889 | 74.8 | 34 | 60.7 | 97 | 91.5 | 4 | 100.0 | 0.000 |
| Foreign | 299 | 25.2 | 22 | 39.3 | 9 | 8.5 | 0 | – | |
Among HIV/HCV cases 52.8% had been infected through injection drug use. In HIV/HBV and HIV monoinfected patients, the main risk factor for viral transmission was sexual exposure (Fig. 1).
.")
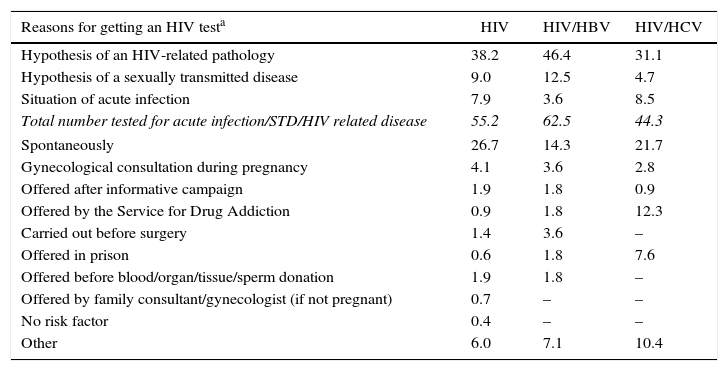
HIV testing was mainly done due to suspicion of a disease or HIV-related clinical signs of acute infection, especially in HIV/HBV patients (62.5%). The test was performed spontaneously due to the perception of the risk of infection by 14.3% of HIV/HBV, 26.7% of HIV monoinfected, and 21.7% of HIV/HCV patients. Moreover, among HIV/HCV patients, 7.6% and 12.3% of the patients performed the test in prison or because it was offered by the Service for Drug Addiction (Table 2).
Reasons for getting an HIV test in HIV, HIV/HBV, HIV/HCV, HIV/HCV/HBV adult patients notified in Tuscany (2009–2013).
| Reasons for getting an HIV testa | HIV | HIV/HBV | HIV/HCV |
|---|---|---|---|
| Hypothesis of an HIV-related pathology | 38.2 | 46.4 | 31.1 |
| Hypothesis of a sexually transmitted disease | 9.0 | 12.5 | 4.7 |
| Situation of acute infection | 7.9 | 3.6 | 8.5 |
| Total number tested for acute infection/STD/HIV related disease | 55.2 | 62.5 | 44.3 |
| Spontaneously | 26.7 | 14.3 | 21.7 |
| Gynecological consultation during pregnancy | 4.1 | 3.6 | 2.8 |
| Offered after informative campaign | 1.9 | 1.8 | 0.9 |
| Offered by the Service for Drug Addiction | 0.9 | 1.8 | 12.3 |
| Carried out before surgery | 1.4 | 3.6 | – |
| Offered in prison | 0.6 | 1.8 | 7.6 |
| Offered before blood/organ/tissue/sperm donation | 1.9 | 1.8 | – |
| Offered by family consultant/gynecologist (if not pregnant) | 0.7 | – | – |
| No risk factor | 0.4 | – | – |
| Other | 6.0 | 7.1 | 10.4 |
HIV/HBV patients presented a worse clinical and immunological picture compared with HIV monoinfected and HIV/HCV patients. HIV viral load of HIV/HBV and HIV/HCV coinfected patients was not significantly different. In HIV/HBV patients the proportions of LP (78.6%) and AHD (64.3%) were higher compared to HIV/HCV (61.3% and 41.5%) and HIV monoinfected patients (55.2% and 39.6%). AIDS was diagnosed in 39.3%, 20.7%, and 7.6% of HIV/HBV, HIV monoinfected and HIV/HCV patients, respectively.
Adjusting for gender, age, nationality, and risk factors, the HIV/HBV patients showed a higher risk to be LP compared to HIV monoinfected patients (OR 3.04; 95% CI: 1.55–5.95). The risk of having AHD was also higher in HIV/HBV patients (OR 2.84; 95% CI: 1.57–5.14) compared to HIV monoinfected patients. No statistically significant difference was found between HIV/HCV and HIV monoinfected patients (Table 3). Compared to HIV monoinfected patients, HIV/HBV patients had a higher risk of AIDS (OR 2.44; 95% CI: 1.35–4.43) while the risk of HIV/HCV patients seemed lower (OR 0.23; 95% CI: 0.10–0.52).
Multivariate logistic regression analysis. Estimate of relative risk for HIV, HIV/HBV, HIV/HCV to be LP, AHD or AIDS. Adult patients notified in Tuscany. 2009–2013.
| Late presenter | Advanced HIV disease | AIDS | |||||||
|---|---|---|---|---|---|---|---|---|---|
| %a | OR | IC 95% | % | OR | IC 95% | % | OR | IC 95% | |
| HIV | 55.2 | 1.00 | – | 39.6 | 1.00 | – | 20.7 | 1.00 | – |
| HIV/HBV | 78.6 | 3.04 | 1.55–5.95 | 64.3 | 2.84 | 1.57–5.14 | 39.3 | 2.44 | 1.35–4.43 |
| HIV/HCV | 61.3 | 1.24 | 0.75–2.05 | 41.5 | 0.81 | 0.49–1.34 | 7.6 | 0.23 | 0.10–0.52 |
Odds ratio and confidence intervals at 95% adjusted by gender, age, nationality, mode of transmission.
To our knowledge, this study shows for the first time that the clinical and immunological features of HIV/HBV coinfected patients are more severe compared to those co-infected with HIV/HCV and HIV monoinfected patients at the time of HIV diagnosis. HIV was diagnosed either in prison or by the Service for Drug Addiction in almost 20% of HCV/HIV coinfected patients, which may have contributed to the less advanced HIV disease in this population. In fact, drug use is the main risk factor for transmission in this group of patients. Moreover, about 15–45% positive for anti-HCV antibodies spontaneously clear the virus.
The HIV/HBV co-infection was common in foreigners and they had both age and risk factors similar to those who were HIV monoinfected. However, these patients had a worse immunological picture at the time of HIV diagnosis compared to HIV/HCV co-infected patients, probably because the sexual transmission was the main risk factor in HIV/HBV coinfected patients, with subsequent less perception of the infection transmission risk, therefore they only performed the test after experiencing HIV-related symptoms. Moreover, they were at higher risk of having LP, AHD, or AIDS compared to HCV coinfected patients. According with these findings, recent studies pointed out that HBV infection complicates the management of HIV infection. In fact, patients with chronic HBV at the time of HIV diagnosis had an impaired CD4 recovery, an accelerated immunologic deterioration, and a significantly higher risk of an AIDS or death event.9,10 This is similar to HIV induced impairment of HBV, which in turn influences negatively the course and progression of HIV disease.
We also found a high prevalence of HBV–HIV coinfection in foreigners. In 1991, Italy initiated universal HBV vaccination for all newborns and 12-year-old adolescents. Since the vaccination programs had a different pace in developing countries, the high prevalence among foreigners could be due to non-compliance with Italy's vaccination program.11
The introduction of blood-screening for HCV in the early 1990s strongly decreased HCV transmission from blood transfusions. Our data also confirm the results of several studies that showed a high prevalence of HCV coinfection in HIV-infected intravenous drug users.6,12,13 Moreover, this co-infection was more prevalent in patients aged 35–59 years, corresponding to those born in the years at major risk for drug abuse. Baby boomers are people born during the post-World War II, approximately between the years of 1946 and 1964. HCV infection and fatty liver disease are more common in the Baby Boomers and may play a more dominant role as they age,14 probably because aging of the baby boomer cohort will soon comprise a large proportion of persons who have used illicit drugs in their lifetimes. A recent cross-sectional study conducted in Brazil showed that the prevalence rate of HIV-HCV coinfection was 6.9% among 848 HIV-infected patients receiving care at reference centers in the Midwest Region of Brazil.15 This also confirms the less advanced disease in these patients, probably due to a higher perceived risk of disease, which could lead them to test earlier. Even after adjusting for gender, age, nationality, and transmission route, we were able to show that HIV/HCV had a lower risk of having AIDS diagnosis at the time of detection of HIV infection compared to HIV monoinfected patients.
HCV screening in HIV-infected patients is highly recommended in order to treat HCV infection when appropriate. Currently, interferon-free treatment regimens are available and they require shorter periods of treatment (3 months). These regimens are free of the associated substantial side effects, and preliminary results suggest that these treatments are also effective in patients with cirrhosis (some for 6 months).16
In conclusion, our data show that both age and risk factors for HIV/HBV coinfected patients are similar to that of HIV monoinfected patients. Moreover, the prevalence of HBV was higher in HIV-infected foreigners compared to HIV-infected Italian patients. Future pathogenesis studies are needed to confirm the higher risk for LP, AHD, and AIDS in HBV coinfected patients. Our data also confirm a higher prevalence of HIV/HCV infections among drug addicts, especially in the 35–59 age group, corresponding to those born in the years considered most at risk for drug abuse. This also suggests that the higher perceived risk of disease leads to earlier HIV testing compared to HIV/HBV patients.
Conflicts of interestThe authors declare no conflicts of interest.
