


Co-infections of hepatitis C virus (HCV) and either human immunodeficiency virus type 1 (HIV-1), human T-cell lymphotropic virus type 1 (HTLV-1) or type 2 (HTLV-2) have been described as having an impact on HCV viremia and subsequent disease progression. HCV load in serum samples from 622 patients (343 males, 279 females; median age 50.8 years) from São Paulo/southeast Brazil was analyzed using the Abbott Real Time HCV assay (Abbott Molecular Inc., IL, USA). Samples were obtained from HCV-monoinfected (n=548), HCV/HIV-1- (n=41), HCV/HTLV-1- (n=16), HCV/HTLV-2- (n=8), HCV/HIV/HTLV-1- (n=4), and HCV/HIV/HTLV-2-co-infected (n=5) patients, and results were compared among the groups and according to sex. The median HCV load in HCV-monoinfected patients was 5.23 log10 IU/mL and 0.31 log10 higher in men than in women. Increases in viral load of 0.51 log10, 0.54 log10, and 1.43 log10 IU/mL were detected in HCV/HIV-1-, HCV/HTLV-1- and HCV/HIV/HTLV-1-co-infected individuals, respectively, compared with HCV-monoinfected counterparts. In contrast, compared to HCV/HIV co-infected patients, HCV/HTLV-2-co-infected patients had an HCV load of 5.0 log10 IU/mL, whereas HCV/HIV/HTLV-2-co-infected patients had a median load 0.37 log10 IU/mL lower. Significant differences in HCV loads were detected, with males and HCV/HIV-1- and HCV/HIV/HTLV-1-co-infected patients presenting the highest values. Conversely, females and HCV/HTLV-2-co-infected patients exhibited lower HCV loads. Overall, HCV viremia is increased in HIV and/or HTLV-1-co-infection and decreased in HTLV-2 co-infection.
Hepatitis C virus (HCV) infection is an important health problem both in Brazil and worldwide because a considerable number of infected patients progresses to chronic liver diseases (cirrhosis and hepatocellular carcinoma) and require liver transplantation.1 In Brazil, mandatory notification of HCV infection has been implemented since 1998. From 1999 to 2015, the Brazilian Ministry of Health (MH) recorded 289,459 cases, 64.2% of which occurred in the southeast region.2 In addition, a cross-sectional population-based survey conducted in Brazil from 2005 to 2009 revealed an overall prevalence of 1.38% and estimated 1.3 million HCV-infected individuals in the country.3
Associations between HCV infection and old age, injected-drug use, sniffed-drug use, hospitalization, lack of sewage disposal, and injection with glass syringes have been described, and these associations depend on the socio-demographic characteristics of patients and regions.3 Located in the southeast region, São Paulo is the most populous and wealthy state in Brazil, where HCV has been detected in 0.9% of individuals aged 10–19 years, and in 1.63% of those aged 20–69 years.3
HCV-infected patients are reported to the Brazilian MH, which provides free universal access to treatment, HCV genotyping and viral load determination.4 Furthermore, the Brazilian MH recommends that HCV loads be measured for diagnosis confirmation and after six months of follow-up. Moreover, in patients without spontaneous HCV clearance and/or in those who have started treatment, genotyping and subsequent viral load measurements are recommended four times a year.4
Human T-cell lymphotropic virus types 1 and 2 (HTLV-1 and HTLV-2) are endemic in Brazil,5 with an estimated 2.5 million individuals infected with HTLV.6
HTLV-1 is associated with at least two diseases of high morbidity and mortality: adult T-cell leukemia/lymphoma (ATLL) and HTLV-1-associated myelopathy/tropical spastic paraparesis (HAM/TSP).5 Despite their endemicity and high morbidity, HTLV-1 or HTLV-2 notification is not compulsory in Brazil.
Human immunodeficiency virus type 1 (HIV-1) is responsible for the acquired immunodeficiency syndrome (AIDS) pandemic; notification is compulsory in Brazilian blood banks since 1988. From 1980 to 2016, the Brazilian MH reported 882,810 HIV/AIDS cases, with 52.3% in the southeast region.7
As all of these viruses share some common routes of transmission/infection, there is a tendency for co-infection.
HIV/HCV co-infection has been associated with poorer outcomes of subsequent diseases.4,8,9 HIV/HTLV-1 co-infection induces rapid progression toward AIDS and death10,11; HIV/HTLV-2 slows the progression toward AIDS.12
Although HCV/HTLV-1/-2 co-infection has been associated with worse outcomes of HCV infection worldwide (higher HCV viremia, lower rate of sustained virological response to α-interferon treatment, increased risk of chronic liver disease, and cancer), this is not the case in Brazil.13 Indeed, in Brazil, HCV/HTLV-1 co-infection has been associated with spontaneous clearance of HCV, and less liver injury.9,13–16
The present study aimed to confirm or refute the positive influence of HTLV-1 on HCV viremia in co-infected patients in Brazil, and to add further information concerning the impact of HIV-1, HTLV-1, and HTLV-2 on HCV viremia in patients from São Paulo.
MethodsStudy populationThe Instituto Adolfo Lutz (IAL), a Public Health Laboratory located in São Paulo city, is a reference laboratory for viral hepatitis, HIV, HTLV-1, and HTLV-2 infections. IAL is responsible for the surveillance of these viruses and to assess trends of infections and co-infections. Blood samples are sent to IAL from several Specialized Health Centers in the state of São Paulo, i.e., STD/AIDS and Viral Hepatitis Centers and Gastroenterology and/or Hepatology Services. A cross-sectional study was conducted using data obtained from serum samples collected from 622 patients analyzed for HCV viral load during the period of June to November 2014 at IAL.
For this study, samples were collected from the following health centers: Gastroenterology Service in the city of São Paulo (n=181); several specialized services of Infectious Diseases, STD/AIDS and Viral Hepatitis, and Gastroenterology and Hepatology outpatients services, located in the Metropolitan area of São Paulo city; in two cities located south of São Paulo (n=124 and n=8, respectively); and in cities situated in the eastern part of the state, up to 200km away from São Paulo city (n=309) (Fig. 1).
Laboratory methods
After performing HCV load measurement using a Real-Time HCV assay (Abbott Molecular Inc., IL, USA), with a lower limit of detection of 12IU/mL, samples were tested for HIV-1, HTLV-1 or HTLV-2 co-infection, as previously described.17
Briefly, anti-HTLV-1/-2 antibodies were detected by an enzyme immunoassay (EIA, HTLV-I/II, Gold ELISA, REM Ind. Com. Ltda, São Paulo, SP, Brazil) and confirmed by line immunoassay (INNO-LIA HTLV-I/II, Fujirebio, Europe N.V., Belgium). HIV-1 infection was evaluated by using an immunochromatographic assay (Rapid Check HIV 1+2, Universidade Federal do Espírito Santo, ES, Brazil) and an enzyme immunoassay (GS HIV-1/HIV-2 Plus O EIA, Bio-Rad Laboratories, USA). All assays were conducted according to the respective manufacturers’ instructions. A prevalence of 7.9% of HIV-1 and 5.3% of HTLV-1/-2 were detected, revealing HTLV-1/-2 infection in patients with hepatitis C, regardless of their HIV-1 status.17
Groups for analyses and data collectionSix groups were categorized according to the results (positive or negative) for the following HIV-1 and HTLV-1/-2 serological assays: HCV monoinfection (n=548); HCV/HIV-1 (n=41), HCV/HTLV-1 (n=16), HCV/HTLV-2 (n=8), HCV/HIV/HTLV-1 (n=4), and HCV/HIV/HTLV-2 co-infection (n=5).
HCV viral loads were abstracted from laboratory records and analyzed according to the type of viral infection or co-infection.
Statistical analysesDifferences in the number of males and females in each group were evaluated statistically using the Chi-square test or Fisher's exact test, as appropriate. HCV loads were log10 transformed and analyzed according to sex and viral infection or co-infection. Prism® Version 5.03 (GraphPad) was used for pairwise comparisons using the Mann–Whitney U-test. Results with a p-value of <0.05 were considered statistically significant.
Ethical reviewThe study was approved by the Ethics Committee for Research of IAL CTC#21I-2016, under Ministry of Health protocol number CAAE – 55837316.0.0000.0059.
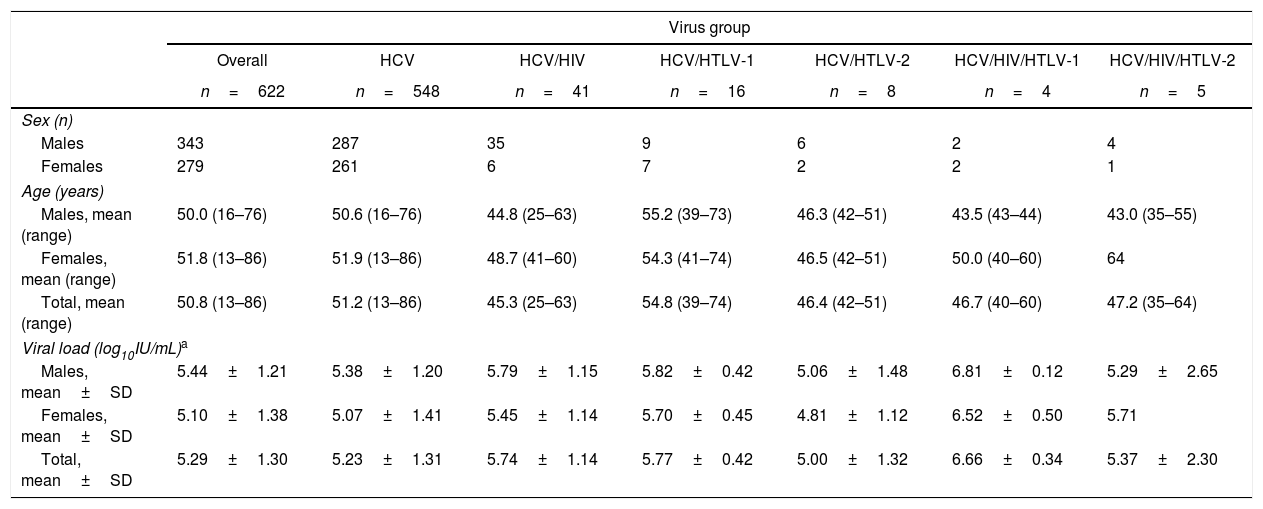
ResultsTable 1 presents the characteristics of the study population (age and sex) as well as the results of HCV viral load for each group.
Characteristics of the study population and results of HCV viral load according to the type of infection and co-infection.
| Virus group | |||||||
|---|---|---|---|---|---|---|---|
| Overall | HCV | HCV/HIV | HCV/HTLV-1 | HCV/HTLV-2 | HCV/HIV/HTLV-1 | HCV/HIV/HTLV-2 | |
| n=622 | n=548 | n=41 | n=16 | n=8 | n=4 | n=5 | |
| Sex (n) | |||||||
| Males | 343 | 287 | 35 | 9 | 6 | 2 | 4 |
| Females | 279 | 261 | 6 | 7 | 2 | 2 | 1 |
| Age (years) | |||||||
| Males, mean (range) | 50.0 (16–76) | 50.6 (16–76) | 44.8 (25–63) | 55.2 (39–73) | 46.3 (42–51) | 43.5 (43–44) | 43.0 (35–55) |
| Females, mean (range) | 51.8 (13–86) | 51.9 (13–86) | 48.7 (41–60) | 54.3 (41–74) | 46.5 (42–51) | 50.0 (40–60) | 64 |
| Total, mean (range) | 50.8 (13–86) | 51.2 (13–86) | 45.3 (25–63) | 54.8 (39–74) | 46.4 (42–51) | 46.7 (40–60) | 47.2 (35–64) |
| Viral load (log10IU/mL)a | |||||||
| Males, mean±SD | 5.44±1.21 | 5.38±1.20 | 5.79±1.15 | 5.82±0.42 | 5.06±1.48 | 6.81±0.12 | 5.29±2.65 |
| Females, mean±SD | 5.10±1.38 | 5.07±1.41 | 5.45±1.14 | 5.70±0.45 | 4.81±1.12 | 6.52±0.50 | 5.71 |
| Total, mean±SD | 5.29±1.30 | 5.23±1.31 | 5.74±1.14 | 5.77±0.42 | 5.00±1.32 | 6.66±0.34 | 5.37±2.30 |
n, number of individuals; IU, international units; SD, standard deviation.
HCV/HTLV-1/-2 co-infection was detected in 33 patients, as follows: in 11 (6.1%) of 181 from the Gastroenterology Service of São Paulo city; in 16 (5.2%) of 309 from cities located in the eastern part of São Paulo State; in 6 (4.5%) of 132 from other services in the surrounding Metropolitan area of São Paulo and from south of São Paulo city.
No difference in relation to age was observed among the groups (p>0.05 in all analyses). Regarding gender, males comprised the majority of HCV/HIV co-infected patients (p=0.0002). Overall, the median HCV load was 5.29 log10 IU/mL, which was 0.34 log10 higher in men than in women. The same profile was observed in the HCV-monoinfected group, which presented a viral load of 5.23 log10 IU/mL, 0.31 log10 higher in men than in women. Viral load were 0.51 log10, 0.54 log10, and 1.43 log10 IU/mL higher in HCV/HIV-1-, HCV/HTLV-1-, and HCV/HIV/HTLV-1-co-infected individuals, respectively, compared to HCV-monoinfected counterparts. In contrast, an HCV load in HCV/HTLV-2-co-infected patients was 5.0 log10 IU/mL (0.23 log10 lower than in HCV-monoinfected patients); in HCV/HIV/HTLV-2-co-infected patients HCV load was 0.37 log10 IU/mL lower than in HCV/HIV-co-infected counterparts (Table 1). Of note, no patient had an undetectable serum viral load, and the current viral load was only determined in 33.3% of patients.
Median viral load results were significantly different between males and females in the overall sample and in the HCV-monoinfected (p=0.0016 and p=0.0147, respectively) group. In addition, median viral load was lower in the HCV-monoinfected than HCV/HIV (p=0.0011), but the HCV/HIV group had lower viral load than the HCV/HIV/HTLV-1 (p=0.0433) group. Although it did not reach statistical significance (p=0.0721), median viral load in the HCV/HIV group had a trend to be higher than in the HCV/HTLV-2 group. Results of p>0.05 were obtained for all other analyses (data not shown). Fig. 2 shows these results, highlighting only the statistically significant associations.
Discussion
The observed difference in the number of individuals with each type of viral infection or co-infection reflects the population characteristics of those visiting each service that sent samples to IAL for analysis. For instance, HCV/HIV co-infection was mostly present in HCV patients attending Infectious Diseases Services (STD/AIDS), whereas no HIV infection was detected in almost all samples from Gastroenterology and/or Hepatology Services of São Paulo (data not shown). Curiously, for the Gastroenterology Service of the city of São Paulo, HCV/HTLV-1/-2 co-infection was detected in 6.1% of patients, though none was HIV-infected. This is of concern, as HTLV serology is not routinely recommended in the clinical management of HCV-infected individuals in Brazil. Nonetheless, the Brazilian MH recommends performing at least one HTLV serology assessment during follow-up of HIV-1 infected individuals.18 Thus, we hypothesize that the patients attending STD/AIDS Centers are more likely to know their HTLV status than are those cared for at other services. Therefore, we suggest including HTLV serology in the battery of tests performed for HCV-infected patients in Brazil, regardless of their HIV-1 status.17
Overall, more males were HCV mono- and co-infected, though there was no significant age difference among groups and between men and women (all p>0.05).
Almost all patients included in this study were over 40 years, in line with the period in which no HCV screening was performed in Brazilian blood banks. In addition, intravenous drugs were frequently used in the country at that time, mostly among HIV-infected men (1980s to 1990s).19–21 Therefore, these patients could have acquired HCV as well as HIV and HTLV-1/-2 infections several years ago by parenteral route [blood transfusion or intravenous drug use (IDU)].
The sexes and ages of HCV-infected patients analyzed in the present study are in agreement with previous Brazilian studies, highlighting the higher rate of HCV-infected individuals of male sex and aged over 40 years.8,9,14–16
Although the present study had no information regarding stage of HCV infection (acute or chronic), treatment, and other characteristics, there was no patient with undetectable viral load. Furthermore, the results for intra-group viral load were very similar (see the standard deviation values, SD), thus allowing comparative analysis among the groups.
Considering the viral load results, one can conclude that men had higher HCV loads, as did HCV/HIV-, HCV/HTLV-1- and HCV/HIV/HTLV-1-co-infected individuals. Lower HCV viral load were detected in women and in HCV/HTLV-2-co-infected individuals from São Paulo. These results are somewhat in accordance with those described in the USA, where females presented lower HCV viremia compared to males.22 These findings are also consistent with the impact of HTLV-1 in HCV infection described in other parts of the world, namely, progression of liver disease and higher HCV load in HCV/HTLV-1-co-infected patients,13 as reported by one study conducted in an adult population of one village endemic for HTLV-1 in Japan (Miyazaki Cohort, Southern Japan).23
Of interest, in a recent study conducted in Iran among IDU, higher baseline HCV viral load were detected in HCV/HIV-co-infected individuals in relation to HCV-monoinfected individuals. The authors suggested that HCV/HIV-co-infected patients should receive more attention and treatment than HCV monoinfected patients.24
Curiously, higher HCV loads in HCV/HIV- and in HCV/HTLV-2-co-infected individuals were detected among IDU from the USA, especially Caucasians.22 These findings contrast with the data obtained in the present study, in which HTLV-2 appeared to reduce HCV viremia, regardless of sex. An explanation for these discordant results among individuals from São Paulo and the USA may be the genetic background of individuals and the HTLV-2 strain circulating in Brazil. Indeed, this strain differs from that circulating in the USA (HTLV-2c and HTLV-2a, respectively).25,26 HTLV-2c has an additional 25 amino acids at the C-terminal end of the regulatory protein Tax, which may have contributed to the results obtained.25,26 Regardless, this hypothesis requires further investigation.
Of interest, when we analyzed the laboratory reports of HCV/HTLV-2-co-infected patients, 23.1% showed HCV clearance in blood during follow-up (data not shown), contrasting with 15.0% of HCV/HTLV-1-co-infected patients (p=0.02). All patients with HCV clearance received standard therapy based on the combination of pegylated-interferon alpha (PEG-IFN) plus ribavirin. In effect, both the low median viral load in HTLV-2-coinfected patients and the large number of patients with HCV clearance during follow-up and treatment agree with the hypothesis of the benefit of HTLV-2c to HCV outcomes.
On the one hand, our findings concerning HCV/HTLV-1-co-infected patients agree with the results from others countries,13 on the other hand, they differ partly from those reported in Brazil concerning the spontaneous clearance of HCV and reduced hepatic injury in HCV/HTLV-1-co-infected patients.9,14–16 One explanation for these discordant results is the characteristics of the study population. The majority of Brazilian studies recruited patients at HTLV outpatient clinics, and this might have introduced bias in the interpretation of results. HTLV-1 infection is more frequently detected in the northeastern region of Brazil, mostly in individuals of African origin.5,6,8,9,15,27 In fact, the majority of Brazilian studies were conducted in Salvador, Bahia, which is a city with the greatest number of African descendants in the country.8,9,15,27
When analyzing HIV/AIDS patients in São Paulo, we detected an association between HIV/HTLV-1/2 infection in black/pardo-colored individuals (OR 2.21, 95% CI 1.21–4.03).21 However, the majority of serum samples were from patients attending specialized services for hepatitis, other than HIV/AIDS or HTLV outpatient clinics.
Thus, one explanation for the discrepant results obtained in São Paulo and other parts of Brazil is the genetic background of patients, as well as the recruited study population. Of note, the population inhabiting São Paulo is of mixed race; the state was colonized by Europeans, Asians, and Middle Easterners, and it also receives migrants from other parts of the country.
Whether the population origin interferes with the obtained results remains to be determined, however we could speculate that the genetic background could increase or decrease HCV viral load, affecting HCV, HIV-1, and HTLV-1 infection outcomes, as previously described.28 In fact, IL28B polymorphisms are associated with spontaneous HCV clearance and sustained virological response.28–30 In conclusion, more studies are needed to confirm or refute the present results, including clinical and laboratory follow-up.
Conflicts of interestThe authors declare no conflicts of interest.
This study was supported in part by grants from FAPESP # 2012/51220-8 and # 2016/03654-0. ACA receives support from CNPq PD # 302661/2015-8. FAA is receiving a master fellowship and KRC a doctoral fellowship, both supported by CAPES. The views expressed are those of the authors and do not reflect the Brazilian Ministry of Health or other institutions/organizations. The funders had no role in the decision to publish or in the preparation of the manuscript.
The authors thank Mirthes Ueda for helpful comments.
