
The aim of the study was to determine the effect of hydrogen peroxide (HP) mouthwash on the incidence of ventilator associated pneumonia (VAP) in patients admitted to the intensive care unit (ICU).
MethodsThis was a randomized clinical trial conducted on 68 patients. The intervention group used 3% HP as mouthwash and the control group used mouthwashes with 0.9% normal saline (NS) twice a day. Data were collected using a questionnaire and the Modified Clinical Pulmonary Infection Score (MCPIS). MCPIS includes five items, body temperature: white blood cell count, pulmonary secretions, the ratio of pressure of arterial oxygen (PaO2) to fraction of inspired oxygen (FiO2), and the chest X-ray. Each of these items scored 0–2. Scores ≥6 were considered as VAP signs. The SPSS-20 software was employed to analyze the data.
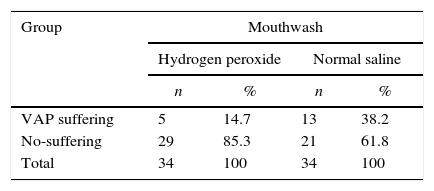
ResultsIn total, 14.7% patients of the HP group and 38.2% patients of the NS group contracted VAP. The risk of VAP in the NS group was 2.60 times greater than that in the HP group (RR=2.60, 95% CI: 1.04–6.49, p=0.0279). The mean±SD MCPIS was calculated as 3.91±1.35 in the HP group and 4.65±1.55 in the NS group, a difference statistically significant (p=0.042). There were no significant differences in the risk factors for VAP between the two groups.
ConclusionHP mouthwash was found more effective than NS in reducing VAP. HP mouthwash can therefore be used in routine nursing care for reducing VAP.
Nosocomial pneumonia is the most common intensive care unit (ICU) infection.1–3 Around 80–90% of patients with nosocomial pneumonia are mechanically ventilated.4,5 Ventilator associated pneumonia (VAP) is the inflammation of the lung parenchyma caused by infection after the patient is connected to the mechanical ventilator.6,7 Therefore, patients with VAP have a tracheal tube inserted or are under tracheostomy or might even be in the process of disconnecting from the ventilator in the 48h preceding the onset of symptoms.6,7 VAP represents a major public health issue in Asian countries and worldwide.8 The prevalence of VAP is 22.5% and 18.2% in general and intensive surgical wards of the hospitals affiliated to Tehran University of Medical Sciences in Iran,9 and 16.2% in China.10 VAP is one of the most common nosocomial infections in Asian countries,11 caused by highly resistant bacterial,8 and a mortality rate ranging from 18.7% to 40.8%.11 Access to appropriate antibiotic therapy for VAP is costly12; moreover, Asian countries exhibit different patterns of epidemiology, etiology, and drug resistance profile compared with Western countries.13
The best way to prevent VAP is to use mouthwash.14 The American Association of Critical-Care Nurses (AACN) (2003) proposed mouthwash not only to bring comfort to the patients, but also as a nursing care for the prevention of VAP.15,16 The AACN guideline recommends to brush the teeth twice a day, swab the mouth every 2–4h, and suction to clear secretions from the mouth.15 Oral rinsing with a solution, gel, and brush, or a combination of these along with aspiration, reduces the risk of VAP in patients under ventilation. Previous studies that have aimed to assess the incidence of VAP have shown no difference between mouthwash and oral care without brushing, with or without the use of mouthwash solution.7 Although some institutions do not follow the AACN recommendations, it is actually oral care that helps preventing VAP.15 Using mouthwash in the patients is one of the main responsibilities of ICU nurses. However, despite the importance of using mouthwash for reducing VAP, its application is often neglected or carelessly performed due to the critical conditions of the patients and their severe physiological deficiencies.15,16
Various solutions are used as mouthwash. Tap water might be plentiful and economical; however, it is a source of nosocomial infections and is therefore not recommended.16,17 The application of NS is restricted due to the dry mouth and patients intolerance.17 The long-term use of povidone–iodine as a mouthwash solution at ICUs is also not recommended due to its absorption, modifications of the normal oral flora and microbial resistance it may cause.18 Sodium bicarbonate solution is a mouthwash that softens the hardened mucosa17 but causes greater bacterial plaque accumulation compared to chlorhexidine. Chlorhexidine is therefore considered an anti-plaque agent with antimicrobial properties that does not lead to bacterial resistance in the oral cavity.1,17,18 Most of the evidence suggests that the use of chlorhexidine is preferred for cardiac surgery patients; yet, its benefits in ICUs are unknown and its routine use is not recommended for all ICU patients.15,17 The Society of Critical Care Medicine and the Centers for Disease Control and Prevention have recommended the use of chlorhexidine mouthwash for cardiac surgery patients and stated that its benefits for other patients are unknown.19 In addition, chlorhexidine has certain side-effects, mainly including tooth discoloration, bitter taste, impaired palate, mucosal damage, oral edema, facilitating tartar build-up above the gum line, and unilateral and bilateral parotid inflammation.20
HP is a colorless liquid with a strong oxidizing activity that has been used as a tooth whitener and anti-plaque agent for over 100 years. Through producing free radicals, this solution has a killing effect on Gram-positive and Gram-negative bacteria – particularly anaerobic bacteria. In addition to its antibacterial properties, at 1.5–3% concentrations, it effectively reduces gingival infections and dental plaque.20 The use of maximum 3% concentrations of HP as a mouthwash has been approved by the American Food and Drug Administration.21 The most common side-effects of 3% and lower concentrations of HP include temporary tooth sensitivity and gingival disorders, which are clinically negligible and do not prohibit the use of HP as a mouthwash.22
During the past decade, a wealth of evidence have confirmed HP safety; today, many oral hygiene centers use HP.22 In another review study, Berry et al. emphasized the need for assessing the effect of HP in preventing VAP.17 Given there are no definitive choice of solutions for this purpose, and considering that the effect of HP solutions has not been studied on the incidence of VAP, and also given the high prevalence of VAP in ICUs, the increasing medical costs associated with it, its mortality rate and the substantial effect of mouthwash in its prevention, conducting a study that seeks to find an effective disinfectant solution for reducing VAP seemed essential. The present study therefore aimed to determine the effect of HP mouthwash on the incidence of VAP in ICU patients.
Type of studySixty-eight patients with endotracheal tube and mechanical ventilation were enrolled in this randomized controlled clinical trial, which was conducted at the medical and at the surgical ICUs, between May 23rd and December 23rd, 2013. The study inclusion criteria consisted of being over the age of 18, having been under mechanical ventilation for over 48h, having had no more than one intubation attempt, no facial or oral trauma, no contra-indications to neither mouthwash use nor to 30° bed head elevation, no history of HP allergies, and no evidence suggesting VAP or aspiration. The study exclusion criteria consisted of having had pneumonia prior to the beginning of the study and in the first 48h of mechanical ventilation, transfer from other departments and the elapse of 24h since the insertion of the tracheal tube, the removal of the tracheal tube for any reason during the 5 days the study was being conducted, and the patient's death or transfer from the internal unit to the surgery ICU and vice versa at any time during the 5 days of the study.
Those who met the aforementioned criteria were selected as study subjects and were randomly assigned to either the intervention group or the control group using block randomization and after matching for age (maximum 5 years difference), type of ICU (medical or surgery), and APACHE II scores (a score difference of 5).23 The requirement for conducting randomized controlled clinical practices with a minimal variation in relation to the need for intensive care services having at their disposal effective protocols for the effective application of oral care and resulting reduction of nosocomial pneumonia.24 Patients were randomly divided into two groups by the use of a coin toss, where heads were assigned to the intervention and tails to the control group.
Data collection instrumentThe present study used a two-part questionnaire for data collection. The first part involved patients’ demographic information, including age, gender, disease severity, occupation, predisposing diseases, reason for admission, the department referring the patient to the ICU, duration of hospital stay, antibiotic use, antihistamine and anti-reflux medication, gastroprokinetic agent and analgesic consumption, Glasgow Coma Scale (GCS), history of smoking and drug abuse, which were abstracted from the patient's file and by questioning their relatives. The second part involved the VAP diagnosis using the MCPIS.
Pugin et al. proposed a score for the diagnosis of VAP known as the Clinical Pulmonary Infection Score (CPIS).25 CPIS is based on both clinical and radiological signs, including temperature, leucocytes count, massive purulent tracheal secretions, chest X-ray, oxygenation (defined as the ratio of partial pressure of arterial oxygen and fraction of inspired oxygen, PaO2/FiO2), and semi-quantitative cultures of tracheal aspirate.26 Each diagnostic sign is scored on a scale of 0–2 points, with 12 being the maximum score and >6 indicating VAP. This score has 93% sensitivity and 100% specificity for the detection of VAP.25 Although Singh et al. introduced a modified CPIS index (MCPIS) by omitting the secretion culture variable, it still represents a valid method for the clinical diagnosis of VAP.27 This index was validated by the American Thoracic Society and the Infectious Disease Society of America.26 The maximum score of MCPIS is 10, with <6 indicating the absence of VAP.28 The MCPIS score of <6 improved the predictive value (area under the curve of 0.89, 81.3% sensitivity, and 86.5% specificity).29
The MCPIS, which examined five items, including body temperature, white blood cell count, pulmonary secretions, the ratio of pressure of arterial oxygen (PaO2) to fraction of inspired oxygen (FiO2), and the chest X-ray. Each patient was given a score of 0–2 for each of these items based on his conditions with 0 indicating normal conditions and 1 and 2 indicating worse and worst conditions, in respective order. A body temperature of 36.5–38.4°C was given the score of 0, 38.5–39°C the score of 1, and temperatures in excess of 39°C the score of 2. White blood cell counts between 4 and 11 thousand were given the score of 0, 11–17 thousand the score of 1, and greater than 17 thousand the score of 2. Normal pulmonary secretions were given the score of 0, and if they exceeded the normal amount, they were given the score of 1 or 2 based on the amount of secretion and the physician's opinion. The PaO2/FiO2 ratio was calculated based on the arterial gases and oxygen percentage set on the mechanical ventilator. Ratios in excess of 200 were given the score of 0 and those lower than 200 the score of 2. The chest X-ray was examined by a pulmonary specialist; if no problems were recognized, the patient received the score of 0, if scattered spots were observed, the score of 1, and if concentrated spots were observed the score of 2. The scores obtained for these five items were added up; aggregate scores below 6 signified the absence of a pneumonia diagnosis and aggregate scores equal to or greater than 6 signified VAP.16,25
Scientific validity and reliability of the data collection instrumentsValidity of the Modified Pulmonary Infection Scale was confirmed using the content validity method and a similar study,16 and its reliability was confirmed on 20 study subjects with the Cronbach's alpha of 0.83. Scores in excess of 6 for the scale were reported as indicating the diagnosis of pneumonia with the sensitivity of 93% and the specificity of 100% and the correlation of 0.8 between the CPIS and secretion culture yielded by bronchoalveolar lavage.30 Singh et al. eliminated the culture and staining steps from the tracheal secretions as it took 2–3 days to produce results and instead proposed the modified CPIS.27 Many studies consider scores of 6 and above in the scale to be appropriate diagnostic indicators of VAP.16,25
MethodsThe first mouthwash application was performed in the first 24h of admission. Conditions of using the mouthwash were similar in both groups, and after washing their hands, the bed head was elevated 30° in order to prevent aspiration of secretions. After wearing sterile gloves, the patient's oral mucosal membrane, tongue and gingiva were washed using 4–6 cotton swabs (depending on the patient's oral health) soaked in 15 cc of 3% HP in the intervention group and in 0.9% NS in the control group. Any excess discharges were collected through suction pumps under similarly equal conditions. Before the application of mouthwash and after elevating the bed head, the tracheal tube and mouth secretions were suctioned out using a green nelaton catheter size 14. The suction nozzle was replaced after each application of the mouthwash. This procedure was repeated twice every day at 8am and 4pm. As pouring NS solution into the tracheal tube contributes to the incidence of pneumonia, it was arranged with the department head nurse to avoid performing this unwanted mistake and a note was affixed to the patient's bed. The tracheal tube cuff was monitored before the application of mouthwash and adjusted in pressure through a syringe if below the normal levels, and the patient's low tracheal tube cuff pressure was recorded in the questionnaire. The tracheal tube cuff pressure was measured by hand by the same nurse throughout the study. The current guidelines do not recommend oral decontamination but recommend the use of mouthwash solutions. The first researcher trained two nurses (one working in the day shift and the other in the afternoon shift) to perform both methods. The mouthwash solutions were prepared by the first researcher and provided to the nurses, who were blinded to their content. The doctor in charge of the patients diagnosed with VAP was also blinded to the content of the mouthwash solution. To provide the same quality of oral care to both groups, one nurse performed the mouthwash applications in the morning and another nurse in the evening. The application of these mouthwash formulas continued for five days.31 Prior to the application of mouthwash study subjects were examined for pneumonia on days 1 and 5 using the MCPIS. Patients scoring below 6 on day 1 entered the study and those scoring greater than 6 on day 5 were diagnosed with VAP.
Data analysisStatistical analyses were performed with SPSS 20.0 software using the Kolmogorov–Smirnov, Mann–Whitney, chi-square, and Fisher exact tests. Relative risk (RR) and 95% confidence interval (CI) were also calculated. p<0.05 was considered as statistically significant.
Ethical considerationsEthical considerations of the study included obtaining permission from the Ethics Committee (92.306537, 19.5.2013) and Registry of Clinical Trials (IRCT201305236318N2), a letter of introduction from the university research deputy and the consent of the hospital and ICU authorities. Full explanations were provided about the study objectives and methods, and written consent was obtained from patients or their relatives after ensuring them of the confidentiality of their data and their right to withdraw from the study.
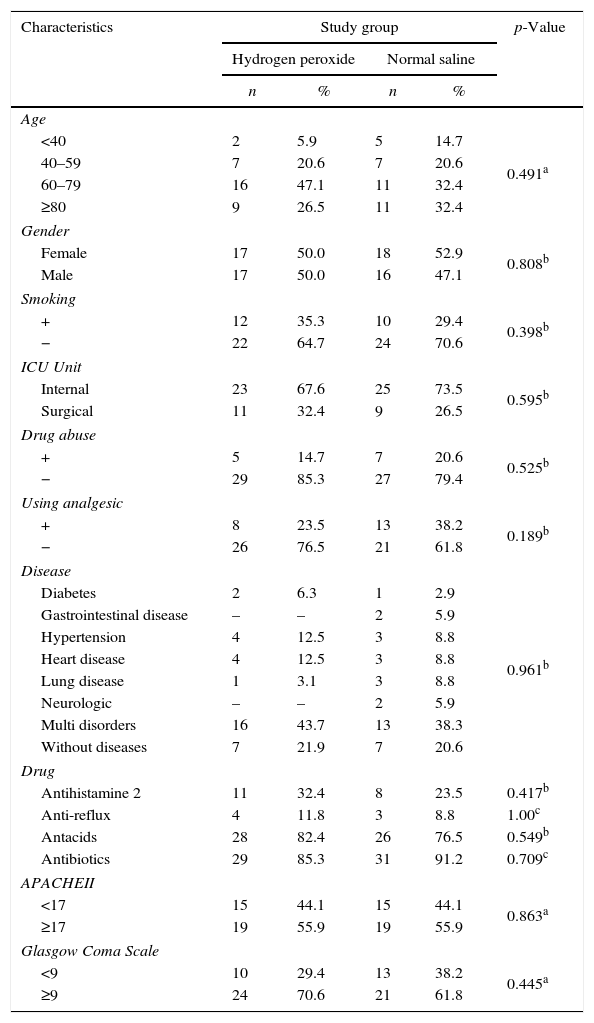
ResultsThe mean±standard deviation (SD) age of patients was 66±15.5 in the HP group and 63.4±20.5 in the NS group (p=0.563). The youngest patient was 19 years old and the oldest 89. The majority (39.75%) of the patients were in the 60–79 age range and the minority (10.3%) were in the below 40 age range; 50% of the patients in the HP group and 47.1% in the NS group were male. There were no significant differences between the two groups in terms of gender (p=0.808); 70.6% of patients were hospitalized in the medical unit and 29.4% in the surgery unit (p=0.595).
The most frequent (50%) causes of hospitalization included the loss of consciousness caused by strokes, cerebral bleeding, and reaction to anesthetics, drug poisoning, Myasthenia Gravis, and unknown causes. The highest APACHE II score was observed in patients with loss of consciousness. The majority of patients in the HP group (43.7%) and 38.3% in the NS group suffered from multiple conditions; however, no significant differences were observed between the two groups (p=0.961). There was not any significant difference between the two groups of HP and NS in terms of type of ICU, predisposing diseases, history of smoking, drug abuse, analgesic drugs, antihistamines 2, anti-reflux, antacids and antibiotics, APACHE II and GCS (Table 1).
Characteristics of hydrogen peroxide and normal saline groups.
| Characteristics | Study group | p-Value | |||
|---|---|---|---|---|---|
| Hydrogen peroxide | Normal saline | ||||
| n | % | n | % | ||
| Age | |||||
| <40 | 2 | 5.9 | 5 | 14.7 | 0.491a |
| 40–59 | 7 | 20.6 | 7 | 20.6 | |
| 60–79 | 16 | 47.1 | 11 | 32.4 | |
| ≥80 | 9 | 26.5 | 11 | 32.4 | |
| Gender | |||||
| Female | 17 | 50.0 | 18 | 52.9 | 0.808b |
| Male | 17 | 50.0 | 16 | 47.1 | |
| Smoking | |||||
| + | 12 | 35.3 | 10 | 29.4 | 0.398b |
| − | 22 | 64.7 | 24 | 70.6 | |
| ICU Unit | |||||
| Internal | 23 | 67.6 | 25 | 73.5 | 0.595b |
| Surgical | 11 | 32.4 | 9 | 26.5 | |
| Drug abuse | |||||
| + | 5 | 14.7 | 7 | 20.6 | 0.525b |
| − | 29 | 85.3 | 27 | 79.4 | |
| Using analgesic | |||||
| + | 8 | 23.5 | 13 | 38.2 | 0.189b |
| − | 26 | 76.5 | 21 | 61.8 | |
| Disease | |||||
| Diabetes | 2 | 6.3 | 1 | 2.9 | 0.961b |
| Gastrointestinal disease | – | – | 2 | 5.9 | |
| Hypertension | 4 | 12.5 | 3 | 8.8 | |
| Heart disease | 4 | 12.5 | 3 | 8.8 | |
| Lung disease | 1 | 3.1 | 3 | 8.8 | |
| Neurologic | – | – | 2 | 5.9 | |
| Multi disorders | 16 | 43.7 | 13 | 38.3 | |
| Without diseases | 7 | 21.9 | 7 | 20.6 | |
| Drug | |||||
| Antihistamine 2 | 11 | 32.4 | 8 | 23.5 | 0.417b |
| Anti-reflux | 4 | 11.8 | 3 | 8.8 | 1.00c |
| Antacids | 28 | 82.4 | 26 | 76.5 | 0.549b |
| Antibiotics | 29 | 85.3 | 31 | 91.2 | 0.709c |
| APACHEII | |||||
| <17 | 15 | 44.1 | 15 | 44.1 | 0.863a |
| ≥17 | 19 | 55.9 | 19 | 55.9 | |
| Glasgow Coma Scale | |||||
| <9 | 10 | 29.4 | 13 | 38.2 | 0.445a |
| ≥9 | 24 | 70.6 | 21 | 61.8 | |
Tests were used:
14.7% of the patients in the HP group and 38.2% of the patients in the NS group acquired VAP. The risk of VAP in the NS group was 2.60 times higher than that in HP group (RR=2.60, 95% CI: 1.04–6.49, p=0.0279) (Table 2). The mean±SD MCPIS was calculated as 3.91±1.35 in the HP group and 4.65±1.55 in the NS group (p=0.042).
DiscussionThe results obtained showed that the use of 3% HP mouthwash significantly reduced the incidence of VAP compared to the use of NS mouthwash (RR=2.60, 95% CI: 1.04–6.49, p=0.0279). The incidence rate of VAP was 14.7% in the HP group. According to a study, using a disinfectant mouthwash solution is the best method for preventing VAP.14 In a study conducted by Hutchins et al., HP was used as mouthwash solution along with other VAP preventative measures. Although their study was conducted without controls and the HP percentage was not specified, the results showed an 89.7% reduction in the incidence of VAP.32
In the present study, the incidence rate of VAP was 38.2% in the NS group. In a study by Seguin et al. saline rinse was compared to usual care (no wash) and found a decrease in VAP.33 Reeve reported that normal saline before tracheal suctioning decreases the incidence of VAP.34 However, the evidence of the effectiveness of normal saline rinsing as a mouthwash is not strong enough. The tendency to cause dry mouth when routinely used as mouthwash has limited its use in critical care units.35
Prevention of ventilator-associated events is a major task.36 Upgrading the oral hygiene in ICU patients may result in reduced incidence of VAP. Although there are various oral care measures for ICU patients proposed in the literature, one cannot identify the most effective measures based on the available evidence.37 Standardization of oral care protocols in ICUs is required in order to improve the quality of oral care provided to ventilated patients.5 Although the use of mouthwash is the best method for reducing VAP, using a disinfectant mouthwash solution is essential for reducing pneumonia. The HP mouthwash examined in the present study has a killing effect on oral anaerobic bacteria and by disinfecting the oral cavity it prevents aspiration of secretions contaminated with bacteria into the lower pulmonary tract, thus reducing VAP. However, the NS solution does not have these properties. The oral health care program have evidently improved oral mucosal health and significantly lowered the occurrence of VAP. The study findings may serve as a pragmatic reference for health care professionals involved in oral health care programs.
Bronchoalveolar lavage (BAL) is a reliable and definitive method for the diagnosis of VAP, which, however, was not used in the present study. It was also neither possible in the present study to examine the mechanical ventilators’ system settings nor assess the patients’ oral health. The results of the present study indicate that use of HP mouthwash is more effective than NS mouthwash in reducing VAP, thereby encouraging future studies to be conducted on the role of HP mouthwash in the incidence of nosocomial pneumonia. It is also recommended for future studies to compare HP to other mouthwash solutions, especially in ICUs, in order to accomplish a more evidence-based care.
ConclusionHP mouthwash was more effective than NS mouthwash in reducing VAP. Nurses can use HP mouthwash in their routine nursing care to reduce the incidence of VAP.
Conflicts of interestThe authors declare no conflicts of interest.
The present paper was part of the master's thesis of Mohammad Reza Razavi, intensive care nursing, Semnan University of Medical Sciences. Hereby, we would like to express our gratitude to the Research and Technology Deputy of Semnan University of Medical Sciences and relevant authorities for their financial and moral support of this study (Grant No. 514). Also we would like to thank the clinical research development unit of Kowsar and Amiralmomenin educational, research and therapeutic center of Semnan University of Medical Sciences for providing facilities to this work. Also we would like to thank the Parisa Hosainkhani and Masoumeh Karkehabadi, nurse specialists, for their sincere help in conducting this study. And last but not least, we would like to show our appreciation to all the participating patients and their families.
