

To describe early-onset neonatal sepsis (EOS) epidemiology in a public maternity hospital in Brasilia, Brazil.
MethodsWe defined EOS as a positive blood culture result obtained from infants aged ≤72 hours of life plus treatment with antibiotic therapy for ≥5 days. Incidence was calculated based on the number of cases and total live births (LB). This is a descriptive study comparing the period of 2012–2013 with the period of 2014–September 2015, before and after implementation of antibiotic prophylaxis during labor for group B streptococcus (GBS) prevention, respectively.
ResultsOverall, 36 infants developed EOS among 21,219 LB (1.7 cases per 1000 LB) and 16 died (case fatality rate of 44%). From 2014, 305 vaginal-rectal swabs were collected from high-risk women and 74 (24%) turned out positive for GBS. After implementation of GBS prevention guidelines, no new cases of GBS were detected, and the EOS incidence was reduced from 1.9 (95% CI 1.3–2.8) to 1.3 (95% CI 0.7–2.3) cases per 1000 LB from 2012–2013 to 2014–September 2015 (p=0.32).
ConclusionsAlthough the reduction of EOS incidence was not significant, GBS colonization among pregnant women was high, no cases of neonatal GBS have occurred after implementation of prevention guidelines.
Early-onset sepsis (EOS) in neonates is a feared and severe complication with high fatality rates. In developed countries, the epidemiology of EOS has been well described with Streptococcus agalactiae, also referred as group B streptococcus (GBS), and Escherichia coli responsible for most of the severe cases.1,2 Additionally, prevention strategies based on GBS screening and intrapartum antibiotic prophylaxis (IAP) to reduce vertical transmission of invasive GBS infection have been implemented for more than a decade.3,4 As a consequence, the incidence of GBS infection in the United States was reduced from 1.7 cases per 1000 live births in the early 1990s to 0.34 cases per 1000 live births after the implementation of antibiotic prophylaxis during labor.3
Nevertheless, the epidemiology of EOS has rarely been described in developing countries, including Brazil. One Brazilian study, published more than a decade ago, described GBS as the pathogen responsible for 50% of culture-proven EOS.5 The incidence of GBS infections in Brazil has ranged from 0.39 and 1.0 per 1000 live births.6–9 The use of IAP has not been adopted as a national strategy to prevent GBS disease, and no data concerning the impact of IAP have been published in the country.
Therefore, we present EOS data from our hospital, which is the largest public maternity hospital in Brasilia, Brazil. We have implemented GBS screening and risk-based IAP in 2014, and herein we compare the epidemiology of EOS in the periods before and after the implementation of IAP.
MethodsSettings and GBS prophylaxis protocolOur hospital is the largest public maternity hospital in Brasilia, central Brazil. It is a regional referral center for preterm-births and neonatal surgery; it has a 30-bed neonatal intensive care unit (NICU) and an intermediate care unit with 16 beds. Before 2014, there was no policy for GBS screening and prophylaxis. IAP was implemented in January 2014, based on the latest Centers for Disease Control and Prevention (CDC) guidelines,3 and consisted of a protocol that instructed the collection of a vaginal-rectal swab for GBS screening for every woman ≥24 weeks of pregnancy admitted to the hospital with premature labor or premature rupture of membranes. Additionally, it recommended IAP for (1) every woman with a positive GBS swab; (2) every woman, regardless of swab result, with a positive urine culture for GBS any time during pregnancy, or with a history of a previous child with GBS sepsis; and (3) every woman with an unknown GBS colonization status, who was in labor <37 weeks of pregnancy or ≥18h of rupture of membranes or with fever (temperature ≥38°C) during labor (Fig. 1). It is important to note that GBS screening during prenatal care was not a policy and that the vast majority of women had an unknown GBS status colonization upon arrival at the maternity hospital.

The swab was collected and immediately placed by the assistant physician in the Todd-Hewitt broth, a selective enrichment broth used to identify GBS, and then forwarded to the microbiology laboratory. After enrichment, GBS was isolated by subcultures on blood agar plates with CAMP-disk test for presumptive identification.
Infant blood cultures were submitted to an automated continuous monitoring system for bacterial detection (Bactec fluorescent series system® Becton Dickinson Microbiology System). Then, an automated panel of bacterial identification (MicroScan Walk-Away® Dade Behring Inc.) was used to identify bacteria species and perform antimicrobial susceptibility test. The laboratory used the Clinical and Laboratory Standards Institute (CLSI) manual for interpretation of minimum inhibitory concentrations (MIC).10
Data collection and statistical analysisWe obtained the positive blood culture data from the microbiology laboratory database for the period of January 2012 to September 2015. Similarly, the number of vaginal-rectal swabs collected in the maternity hospital and their positivity rate after the implementation of the protocol, from January 2014 to September 2015 were also abstracted.
EOS was defined as isolation of a pathogen from blood culture samples drawn within 72h of birth plus antibiotic treatment for ≥5 days or death <5 days while on antibiotic treatment. Coagulase-negative staphylococci (CoNS) grown alone in a single culture bottle were considered contaminants.
Patients’ records were reviewed, and maternal and infant information was collected. The maternal information included gestational age, time of rupture of membranes, presence of intrapartum fever, diagnosis of chorioamnionitis, type of delivery, status of GBS colonization, IAP treatment, and antibiotics received. The infants’ information included date of birth, date of NICU admission, sex, birth weight, and outcome (death or discharge from hospital). Antibiotic susceptibility data were analyzed, if available.
The incidence of EOS was calculated using the number of EOS divided by the numbers of live births (LB) during the period of study. We analyzed the data descriptively, using proportions for discrete variables and the median for continuous variables. The data were examined overall and between two periods: before (2012 and 2013) and after (2014 and 2015) the implementation of the GBS prevention protocol. We used Chi-square test and a 95% confidence interval (95% CI) to compare the EOS incidence rates between these two periods. We also compared data between infants infected with GBS and E. coli.
ResultsPathogens and infection ratesDuring 2012–2013, there were 26 cases of EOS and 13,627 LB, an incidence of 1.9 per 1000 LB (95% CI 1.3–2.8); 12 infants died, a fatality rate of 46%. During 2014–September 2015, there were 10 cases of EOS and 7592 LB, an incidence of 1.3 per 1000 LB (95% CI 0.7–2.3); 4 infants died, a fatality rate of 40%. Thus, for the whole period of study there were 36 cases of EOS and 21,219 LB, an incidence of EOS of 1.7 per 1000 LB (95% CI 1.2–2.3), and a total of 16 deaths, an overall fatality rate of 44%. There was no significant difference in the incidence of EOS between the two periods (p=0.32).
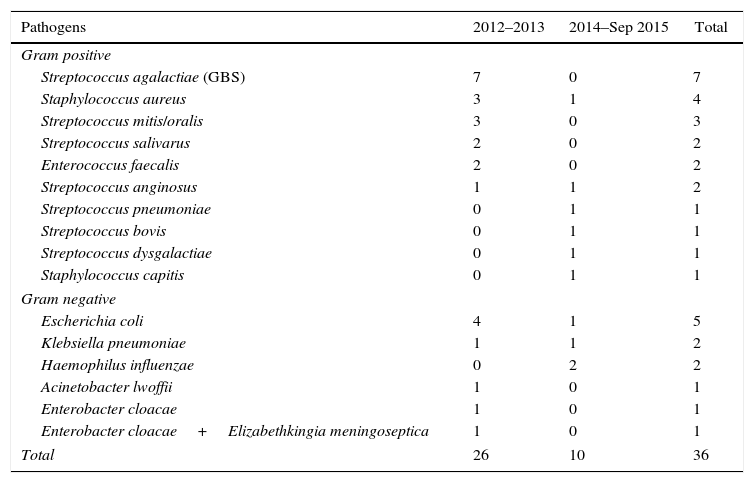
The distribution of pathogens isolated during the study period is presented in Table 1. GBS was the main pathogen isolated from 36 infants, but remarkably no new cases of GBS have been isolated since the implementation of IAP. E. coli was the second most frequently isolated pathogen, followed by Staphylococcus aureus, other Streptococcus species, and Enterococcus faecalis among Gram positive bacteria and other enteric bacilli and Haemophilus influenza among Gram negative bacteria. There was only one infant with more than one microorganism grown in culture. There were 12 blood cultures with CoNS, but only one included as the remaining were considered contaminants.
Distribution of pathogens isolated from early-onset neonatal sepsis during 2012–2013 and 2014–September 2015, Brasilia, Brazil.
| Pathogens | 2012–2013 | 2014–Sep 2015 | Total |
|---|---|---|---|
| Gram positive | |||
| Streptococcus agalactiae (GBS) | 7 | 0 | 7 |
| Staphylococcus aureus | 3 | 1 | 4 |
| Streptococcus mitis/oralis | 3 | 0 | 3 |
| Streptococcus salivarus | 2 | 0 | 2 |
| Enterococcus faecalis | 2 | 0 | 2 |
| Streptococcus anginosus | 1 | 1 | 2 |
| Streptococcus pneumoniae | 0 | 1 | 1 |
| Streptococcus bovis | 0 | 1 | 1 |
| Streptococcus dysgalactiae | 0 | 1 | 1 |
| Staphylococcus capitis | 0 | 1 | 1 |
| Gram negative | |||
| Escherichia coli | 4 | 1 | 5 |
| Klebsiella pneumoniae | 1 | 1 | 2 |
| Haemophilus influenzae | 0 | 2 | 2 |
| Acinetobacter lwoffii | 1 | 0 | 1 |
| Enterobacter cloacae | 1 | 0 | 1 |
| Enterobacter cloacae+Elizabethkingia meningoseptica | 1 | 0 | 1 |
| Total | 26 | 10 | 36 |
All seven GBS isolates were sensitive to penicillin, ampicillin, and vancomycin; they were not tested for clindamycin susceptibility. All five E. coli isolates were resistant to ampicillin and sensitive to third generation cephalosporins; one isolate was gentamicin resistant. No S. aureus was methicillin resistant and no E. faecalis was vancomycin resistant.
Maternal and neonatal clinical featuresAll 36 infants developed symptomatic illness (required blood pressure support or had respiratory distress) of EOS during the period of study; all received ampicillin, penicillin, or cefazolin with gentamicin. Eighteen (50%) were male and 19 (53%) were born through vaginal delivery. Twenty-nine (81%) were preterm (<37 weeks of gestation); the median gestational age was 31 weeks (24–41 weeks). Twenty-one (58%) were ≤1500g; the median birth weight was 1307.5g (470–3800g).
Eighteen (50%) pregnant women had rupture of membranes at delivery. For the other 18 pregnant women, with rupture of membranes before delivery, the median duration of membrane rupture was 72h (1h to 42 days). Overall, 14 (39%) had a period of rupture of membranes longer than 18h. Seven (19%) pregnant women had fever or a diagnosis of presumed chorioamnionitis during labor.
Implementation of GBS prophylaxisDuring 2012–2013, among the 26 pregnant women who had an infant with EOS, none of the women had a vaginal-rectal swab result at labor. According to the latest guidelines,3,4 when considering the unknown status of GBS colonization, 21 (81%) women met the criteria for receiving IAP (12 had premature labor; six had premature labor and rupture of membranes ≥18h; two had premature labor, rupture of membranes ≥18h and fever during labor; and one had term labor and rupture of membrane ≥18h). However, only three (11%) women received antibiotics during labor: two women received clindamycin because of presumed chorioamnionitis, and one received ampicillin and azithromycin for prolonged premature rupture of membranes.
From 2014, the IAP protocol was implemented, and until September 2015, 305 vaginal-rectal swabs were collected from women admitted with preterm labor and 74 (24%) were positive. Out of 10 pregnant women who had an infant with EOS, only one had a vaginal-rectal swab collected that turned out negative. However, the result was known after delivery. Only one woman had a term labor with unknown GBS colonization status, no risk factors for EOS and thus, did not have indications for IAP. Therefore, nine (90%) women should have received IAP, according to the protocol (three had premature labor; one had premature labor and rupture of membranes ≥18h; four had premature labor, rupture of membranes ≥18h and fever during labor; and one had premature labor and fever during labor); however, only five (55.5%) received antibiotics during labor: four received clindamycin for presumed chorioamnionitis, and one received ampicillin as prophylaxis, according to protocol, because she had a preterm labor and rupture of membranes ≥18h.
Group B Streptococcus and E. coliThe total number of infants with GBS infection was seven with an incidence rate of infection during 2012–2013 was 0.51 per 1000 LB or 0.33 per 1000 LB for the whole period of study. No case of EOS due to GBS was detected after the implementation of the IAP protocol. Four (57%) infants were preterm; the median birth weight among GBS infected infants was 2751g (569–3800g). Three infants died, a fatality rate of 43%.
The total number of infants with E. coli infection was five with an incidence rate of infection with E. coli was 0.23 per 1000 LB during the whole period of study. All infants were preterm; the median birth weight among infants infected with E. coli was 1270g (855–2020g). Four infants died, a fatality rate of 80%.
DiscussionThis analysis of a regional referral maternity hospital in Brazil with approximately 20,000 LB shows that the burden of EOS is concentrated among preterm infants. The incidence density of culture proven EOS was 1.7 cases per 1000 LB and the fatality rate was 44%, figures that are higher than those observed in developed countries. EOS incidence density was 0.98 per 1000 LB in the United States2 and 0.9 per 1000 LB in England.11
GBS and E. coli have been the predominant causative microorganisms of EOS, but in this study it corresponded to only a third of cases and almost one half of deaths. Other microorganisms, especially Gram positive bacteria, such as S. aureus, other Streptococcus species, and E. faecalis corresponded to a significant share of cases of EOS in our study. Although Staphylococcus and other Streptococcus species are viewed as possible contaminants, all the infants who had blood cultures with these pathogens, presented clinical or laboratory findings suggestive of infection and received antibiotics. As the importance of CoNS as an EOS pathogen remains controversial, we only considered CoNS as the cause of EOS in the case of one infant who had more than one culture growing CoNS. It is worthy to note that there was no case of Listeria monocytogenes.
The strategy of IAP in developed countries has reduced the incidence of EOS by reducing the cases of GBS. The incidence of GBS in our study (0.51 per 1000 LB), before the implementation of IAP, is within the range of previous Brazilian studies,6–9 but higher than the incidence observed in developed countries, more than a decade after IAP implementation.3,4 We found a positive vaginal-rectal swab prevalence of 24%. This is similar to the range observed in other Brazilian studies of 17.9–27.6%12–14 and the prevalence of 26% observed in the United States.15 Despite this high rate of women with colonization, screening of GBS during prenatal care and IAP during labor is not a national policy in Brazil. During the period of study, more than 80% of women who had an infant with EOS should have received IAP, according to the latest American and European guidelines,3,4 but only 11% of women during 2012–2013 and 55.5% of women during 2014–September 2015, respectively, received IAP. These were missed opportunities for GBS prophylaxis in general, and for preterm labor in particular; antibiotics were more likely to have been prescribed when there was a presumed diagnosis of chorioamnionitis or a long period of membrane rupture. A Brazilian study had already revealed a 57% inappropriate compliance with the IAP protocol.16 Nevertheless, we observed 18 months following the implementation of the IAP protocol, no new cases of GBS have appeared, and the crude EOS incidence has been reduced.
The rational choice of antibiotics for the infant with presumed infection requires review of antibiotic susceptibility of the predominant organisms that cause the disease at a local level. Ampicillin and gentamicin are the recommended empiric antibiotics for the infant at risk of EOS. In our study, all the GBS were sensitive to ampicillin or penicillin, but one out of five E. coli infections was resistant to gentamicin. This finding is worrisome because previous studies have already shown that E. coli has become the most frequent pathogen among preterm infants, who are at the highest risk of severe disease and death.17–19 The incidence of E. coli (0.23 per 1000 LB) in our study is very close to that observed in the United States (0.28 per 1000 LB).2 The median birth weight of infants infected with E. coli was lower than that observed in infants infected with GBS, with a higher fatality rate. Data from developing countries have already reported 13% gentamicin resistance among E. coli neonatal infections.20
Among limitations of the present study, it did not have an uninfected comparison group to assess risk factors and GBS prevention strategies more broadly. Additionally, we have a relative small sample size for an unusual outcome, culture-proven EOS, and a short period of time after implementation of IAP strategy. These factors may explain why we did not find a significant difference between the EOS incidences for the two periods of study. Moreover, our results are ecological findings, and it is not possible to affirm that the reduction in GBS infections was caused only by the IAP protocol. We also had limited external validity because this study was carried out in only one single regional maternity hospital. Different situations may exist in Brazil because it is such a diverse country. Larger studies, including multiple centers, longer time periods, and a different design controlling for confounding variables are necessary to better describe the epidemiology of EOS and to evaluate the impact of IAP strategy in Brazil.
In conclusion, EOS incidence in the studied scenario seems higher than that observed in developed countries. EOS is concentrated among preterm infants and GBS and E. coli are the main pathogens of neonatal infection. Although we did not find a significant difference in EOS incidence before and after the implementation of IAP in our hospital, the EOS incidence was reduced and no new cases of GBS were observed. Evidence-based strategies to reduce the burden of EOS should be implemented, along with efforts to decrease preterm birth rates and to reduce the number of deaths associated with these infections.
Conflicts of interestThe authors declare no conflicts of interest.
We thank the hospital microbiology laboratory for providing the culture data and the obstetric and NICU staff for supporting the implementation of a GBS prevention protocol.
