



Human cytomegalovirus is a major cause of morbidity in kidney transplant patients.
ObjectivesWe aimed to study viral replication and serological response in the first months post kidney transplant in patients undergoing universal prophylaxis or preemptive therapy and correlate the findings with the clinical course of Human cytomegalovirus infection.
Patients and methodsIndependent from the clinical strategy adopted for managing Human cytomegalovirus infection, prophylaxis versus preemptive therapy, the pp65 antigenemia assay and serological response were assessed on the day of transplantation, and then weekly during the first three months of post-transplant.
ResultsFrom the 32 transplant recipients, 16 were positive for pp65 antigenemia, with a similar incidence rate in each group. There were no positive results in the first three weeks of monitoring; the positivity rate peaked at week eight. There was a trend for a higher and earlier frequency of positivity in the universal prophylaxis group in which the course of the Human cytomegalovirus infection was also more severe. Despite the differences in clinical picture and in the initial immunosuppressant schedule, the serological response was similar in both groups.
ConclusionRoutine monitoring during the first three post-transplant months has a positive impact on the early detection of Human cytomegalovirus viral replication allowing for timely treatment in order to reduce morbidity of the disease. The strategy of universal therapy employing intravenous ganciclovir was associated to a worse clinical course of the Human cytomegalovirus infection suggesting that the use of >10 cells/2×105 leukocytes as a cut-off in this setting may be inappropriate.
Human cytomegalovirus (HCMV), a DNA virus, member of herpesviridae family, is one of the major problems associated with organ transplants, directly affecting clinical outcomes and mortality.1–4 In this context, different strategies for monitoring, prevention, and treatment have been applied.5 In several centers, the HCMV screening and monitoring is generally performed using assays for viral biomarkers identification, such as phosphoprotein 65 (pp65) or viral DNA by polymerase chain reaction (PCR).6–8
In preemptive therapy, diagnostic tests are usually performed weekly to guide therapeutic decisions, based on previously defined cut-off. In high risk patients, however, universal prophylaxis has been used, with antiviral drugs administered immediately after transplantation, usually for at least three months.9,10
In transplant recipients undergoing universal prophylaxis screening is not usually performed, and data on potential early replication are unknown. However, it has been established that late disease, following completion of treatment with antiviral drugs, is more likely to occur in this group.11,12 In view of that, some centers use monitoring strategy similar to preemptive protocol after ending treatment.13,14 The objective of the present study was to study viral replication and serological response in the first three months after kidney transplantation in patients undergoing universal prophylaxis or preemptive therapy and correlate the findings with the clinical course of HCMV infection.
Patients and methodsBlood samples of patients undergoing kidney transplantation at the Nephrology Division of a University Hospital were analyzed, from April 2014 (a time when pp65 assay was implemented in our center) to September 2015. This was an observational, prospective, longitudinal study, which analyzed the HCMV replication profile by pp65 antigenemia assay, with internal validation by qPCR assay. In addition, serum levels of anti-HCMV immunoglobulins were quantified. Clinical findings and other laboratory test results were obtained from patients’ charts. The research protocol was approved by the Research Ethics Committee of the Medical School (CAAE: 18768213.1.0000.5243).
Irrespective of the clinical strategy adopted, the monitoring consisted in detection of viral replication in neutrophils infected by HCMV on the day of transplantation and weekly during the first three months. An additional evaluation was conducted at the end of the sixth month post-transplantation. Patients were grouped according to the type of the strategy adopted (preemptive therapy vs. prophylactic therapy).
The pp65 assay was performed by indirect immunofluorescence using Brite™ Turbo kit (IQ Products, Groningen, Netherlands) following the manufacturer's instructions. Results were expressed as the number of positive cells per 2×105 leukocytes. Sample processing and analysis were performed in a blinded fashion by the laboratory staff and the reports were made available on the electronic chart system of the hospital.
Quantification of anti-CMV IgM and IgG was performed using the commercial kits Architect CMV IgG Reagent and Architect CMV IgM Reagent, respectively (Abbott, Ireland), using a HCMV lysate (strain AD169) in a chemiluminescent microparticles immunoassay. The serum levels of anti-HCMV immunoglobulins (IgM and IgG) was measured on the day of transplantation and weekly during the first three months. An additional evaluation was conducted at the end of the sixth month post-transplantation.
The type of strategy (preemptive or universal) was chosen at the discretion of the medical assistants. In case of preemptive therapy, intravenous ganciclovir was initiated when at least 10 positive cells by 2×105 leukocytes (cut-off) were identified in the pp65 assay. In prophylactic therapy, antiviral treatment with ganciclovir was administered soon after transplantation, and maintained for three consecutive months, according to the following criteria: donor CMV IgG positive with CMV IgG negative receptor; donor>60 years; serum creatinine of deceased donor >1.5mg/dL; or whenever the induction therapy was based on thymoglobulin.
Universal prophylaxis with intravenous ganciclovir (5mg/kg) was implemented according to previous institutional protocol: P.O. 1 to P.O. 14, twice a day; P.O. 15 to P.O. 30, three times a week; P.O. 31 to P.O. 60, twice a week, and P.O. 61 to P.O. 90, once a week. The dose of ganciclovir was adjusted to the patient's renal function.
The results were expressed as mean±SD. Differences between groups were analyzed by unpaired Student's t test or Mann–Whitney, according to the distribution pattern. Frequencies were compared using Fisher's exact test. p values <0.05 were considered statistically significant. Statistical analysis was performed using 5.0 GraphPad Prism program.
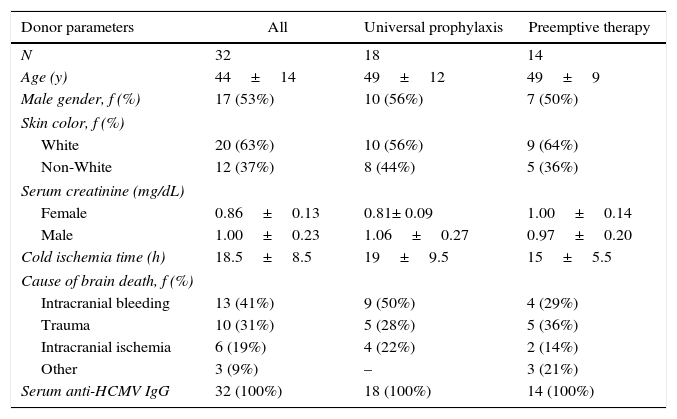
ResultsThirty-two successful kidney transplants were performed during the study period. Baseline characteristics of donors are shown in Table 1. Their mean age was 44±14 years. Intracranial bleeding (41%) was the main cause of death, and all were seropositive for HCMV. The mean cold ischemia time was 18.5±8.5hours and there were no significant differences when comparing the characteristics of donors whose organs were allocated to recipients undergoing universal prophylaxis or preemptive therapy.
Baseline characteristics of kidney donors.
| Donor parameters | All | Universal prophylaxis | Preemptive therapy |
|---|---|---|---|
| N | 32 | 18 | 14 |
| Age (y) | 44±14 | 49±12 | 49±9 |
| Male gender, f (%) | 17 (53%) | 10 (56%) | 7 (50%) |
| Skin color, f (%) | |||
| White | 20 (63%) | 10 (56%) | 9 (64%) |
| Non-White | 12 (37%) | 8 (44%) | 5 (36%) |
| Serum creatinine (mg/dL) | |||
| Female | 0.86±0.13 | 0.81± 0.09 | 1.00±0.14 |
| Male | 1.00±0.23 | 1.06±0.27 | 0.97±0.20 |
| Cold ischemia time (h) | 18.5±8.5 | 19±9.5 | 15±5.5 |
| Cause of brain death, f (%) | |||
| Intracranial bleeding | 13 (41%) | 9 (50%) | 4 (29%) |
| Trauma | 10 (31%) | 5 (28%) | 5 (36%) |
| Intracranial ischemia | 6 (19%) | 4 (22%) | 2 (14%) |
| Other | 3 (9%) | – | 3 (21%) |
| Serum anti-HCMV IgG | 32 (100%) | 18 (100%) | 14 (100%) |
Mean±SD. No statistically significant was found for any of the parameters when comparing universal prophylaxis versus preemptive therapy.
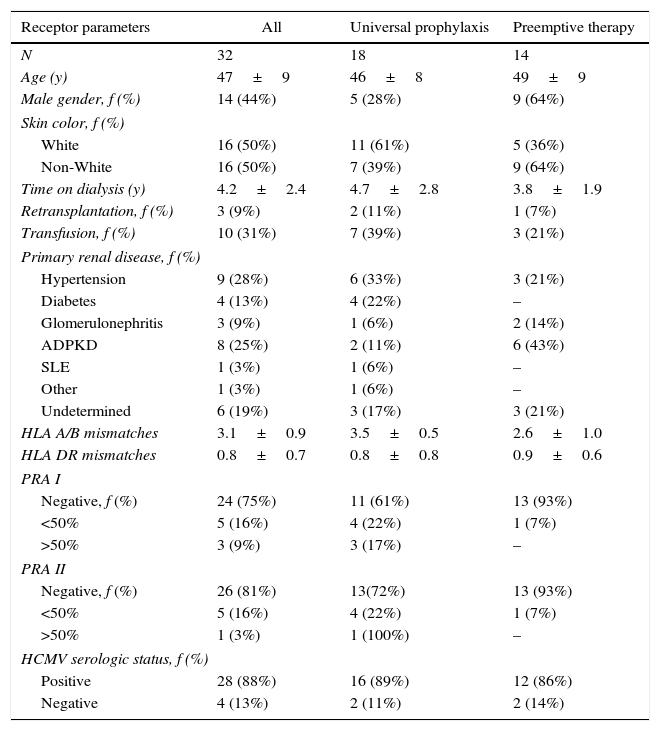
Out of 32 recipients (44% male, 50% white), 18 received universal prophylaxis and 14 preemptive therapy. Baseline characteristics of recipients are shown in Table 2. Again, no statistically significant differences were found when comparing baseline parameters between groups.
Baseline characteristics of recipients, according to the strategy adopted for managing HCMV post kidney transplantation.
| Receptor parameters | All | Universal prophylaxis | Preemptive therapy |
|---|---|---|---|
| N | 32 | 18 | 14 |
| Age (y) | 47±9 | 46±8 | 49±9 |
| Male gender, f (%) | 14 (44%) | 5 (28%) | 9 (64%) |
| Skin color, f (%) | |||
| White | 16 (50%) | 11 (61%) | 5 (36%) |
| Non-White | 16 (50%) | 7 (39%) | 9 (64%) |
| Time on dialysis (y) | 4.2±2.4 | 4.7±2.8 | 3.8±1.9 |
| Retransplantation, f (%) | 3 (9%) | 2 (11%) | 1 (7%) |
| Transfusion, f (%) | 10 (31%) | 7 (39%) | 3 (21%) |
| Primary renal disease, f (%) | |||
| Hypertension | 9 (28%) | 6 (33%) | 3 (21%) |
| Diabetes | 4 (13%) | 4 (22%) | – |
| Glomerulonephritis | 3 (9%) | 1 (6%) | 2 (14%) |
| ADPKD | 8 (25%) | 2 (11%) | 6 (43%) |
| SLE | 1 (3%) | 1 (6%) | – |
| Other | 1 (3%) | 1 (6%) | – |
| Undetermined | 6 (19%) | 3 (17%) | 3 (21%) |
| HLA A/B mismatches | 3.1±0.9 | 3.5±0.5 | 2.6±1.0 |
| HLA DR mismatches | 0.8±0.7 | 0.8±0.8 | 0.9±0.6 |
| PRA I | |||
| Negative, f (%) | 24 (75%) | 11 (61%) | 13 (93%) |
| <50% | 5 (16%) | 4 (22%) | 1 (7%) |
| >50% | 3 (9%) | 3 (17%) | – |
| PRA II | |||
| Negative, f (%) | 26 (81%) | 13(72%) | 13 (93%) |
| <50% | 5 (16%) | 4 (22%) | 1 (7%) |
| >50% | 1 (3%) | 1 (100%) | – |
| HCMV serologic status, f (%) | |||
| Positive | 28 (88%) | 16 (89%) | 12 (86%) |
| Negative | 4 (13%) | 2 (11%) | 2 (14%) |
Mean±SD. HCMV, human cytomegalovirus; HLA, human leukocyte antigen; PRA, panel reactive antibody. Again, no statistically significant was found for any of the parameters when comparing universal prophylaxis versus preemptive therapy.
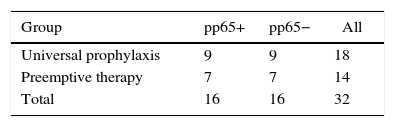
The pp65 antigenemia assay was performed weekly, for six months post-transplant. Sixteen patients were found to be positive for pp65 antigenemia, with a similar incidence between groups (Table 3). The time-line occurrence in weeks of positive cases is depicted in Fig. 1. There were no positive results in the first three weeks of monitoring and the frequency of positivity peaked on week eight. Six month post-transplant only one patient relapsed after three negative evaluations. When comparing the positivity rate along the weeks between the study groups (Fig. 2), there was a trend for a higher and earlier frequency of positivity among those on universal prophylaxis than in those on preemptive therapy. In addition, the positivity tended to last longer in the universal prophylaxis group (4.11±1.83 weeks vs. 2.71±0.95 weeks, p=0.090).
 in kidney transplant patients along the study period.")
.")
From the nine positive patients on universal prophylaxis (mean age of 46.2±9.2 years), three were male. All of them had gastrointestinal manifestations, and in three the virus was also identified by immunohistochemistry in kidney biopsies. One patient was considered clinically resistant to ganciclovir by clinicians and managed with immunoglobulin. Hemophagocytic lymphohistiocytosis was diagnosed in one case. Two of positive cases had a severe form of the disease with a fatal course. From the seven positive patients on preemptive therapy (mean age 51.4±10.5 years), five were male. Here, every positive patient remained asymptomatic.
The mean number of cells of the positive patients and the serological response to HCMV infection are shown in Fig. 3. A significant difference in the number of positive cells/2×105 leukocytes between groups in favor of universal prophylaxis was found (123±423 vs. 23±87, p<0.01). No difference was observed between groups regarding serum levels of either IgG or IgM anti-HCMV.
Discussion and IgM and IgG levels (gray and black columns, respectively) during the study period in kidney transplant patients on universal prophylaxis (Panel A) or preemptive therapy (Panel B).")
HCMV infection is a major concern in kidney transplantation especially during the first three months of post-transplant when higher doses of immunosuppressant are required.15 The profile of both pp65 antigenemia and serological studies were evaluated under universal prophylaxis or preemptive therapy, and the clinical courses of the two groups were compared. The positivity of pp65 antigenemia test can precede clinical symptoms; therefore, it is a useful tool to promptly support clinical decisions and has been considered the gold standard for monitoring HCMV viral replication in solid organ transplant recipients.9,16,17
The mean age of the donors was similar to other studies,18,19 and the positivity rate of IgG anti-HCMV was 100%. More importantly, the analyzed parameters did not differ between groups. The mean age of recipients was also in the range reported by most of the studies.20–22 The profile of the underlying disease was comparable to that described by the Brazilian census of dialysis but with a high percent of ADPKD patients.23 As expected, the proportion of sensitized patients tended to be higher in the universal prophylaxis group.
Consistent with the reported frequency of HCMV infection in the renal transplant population (30–70%),24,25 the overall frequency of HCMV infection in our sample was 50%. Unexpectedly, the rate of HCMV infection in universal prophylaxis and preemptive therapy was the same.
The first positive patient for pp65 antigenemia in our study was detected at week 4, in line with previous reports.16,26 The peak of affected patients occurred at week 8. In some way surprising, the first positive patient was on universal prophylaxis. Indeed, the positivity rate was higher in the first weeks as well as in the last weeks of the study in the group on universal prophylaxis compared to those on preemptive therapy. It should be pointed out that HCMV infection was more severe in those on universal prophylaxis resulting in two fatalities. In the preemptive therapy group, none of the patient had symptoms. Accordingly, the number of infected cells and the duration of positivity were both higher in the universal prophylaxis group. Interestingly, despite the differences in clinical picture and in the initial immunosuppressant schedule, the serological response, as evaluated by the serum levels of specific IgG and IgM, was similar in both groups.
There is almost a consensus in the literature regarding a higher incidence of HCMV following the end of the universal prophylaxis period.27,28 In view of that the period of prophylaxis initially recommended as three months was extended to six months.9 However, if universal prophylaxis is more effective than preemptive therapy in terms of the prevention of the infection and its morbidity is a matter of controversy. The use of different drugs, protocols and routes of administration for universal prophylaxis with potential different results may add some fuel to the debate. In a recent meta-analysis, ganciclovir was found to be comparable to either valganciclovir or valacyclovir regarding the prevention of CMV disease.28 In the present study, universal prophylaxis, when implemented with intravenous ganciclovir, was found to be inferior to preemptive therapy: the rate of HCMV infection was not reduced and the morbidity of the infection was substantially higher with universal prophylaxis. The explanation for the particularities of the clinical course of HCMV infection under the two management strategies is uncertain but two possibilities could be proposed. Patients under universal prophylaxis underwent more aggressive immunosuppression, which may have impaired their immune response against HCMV. In addition, the use of suboptimal doses of intravenous ganciclovir may have perturbed the process of leukocyte invasion by the virus. As a result, an underlying HCMV infection could remain unrevealed and the diagnosis would only be made in a relatively advanced stage of the disease. In this circumstance, the use of more than 10 cells as a cutoff could be inappropriate. We wonder if adopting 1 cell/2×105 leukocytes as a cutoff for a positive test, as already recommended in other solid organ transplantation,7,29 would have changed the course of disease of those on universal prophylaxis.
Reports using intravenous ganciclovir as universal prophylaxis are scarce in the literature since oral administration of drugs is the preferred route in this setting. However, consistent with our findings, a study with intravenous ganciclovir as universal therapy in lung transplantation reported a rate of 68% of HCMV infection in the first year post-transplant.30 Perhaps not accidently, the study was also carried out in our country, in which oral drugs for HCMV prophylaxis are not made available by the public health system. Considering the mentioned specificity of the present study, our findings cannot be used to argue the concept that universal prophylaxis with oral drugs reduces and delays HCMV infection.18,21,31 It does suggest though that when implemented using intravenous ganciclovir, universal prophylaxis does not seem to be warranted in light of our findings.
In conclusion, the present study reiterate that routine monitoring during the first three post-transplant months has a positive impact on early detection of HCMV replication allowing timely treatment to reduce the morbidity of the disease. The strategy of universal therapy employing intravenous ganciclovir was associated to a more severe clinical course of HCMV infection allowing us to think that the use of >10 cells/2×105 leukocytes as a cutoff in this setting may be inappropriate. Further studies, with larger sample sizes, may be needed to confirm our results.
FundingSupport from CAPES and FAPERJ, E-26/111.225/2013.
Conflict of interestThe authors declare no conflicts of interest.
The authors thanks of Andrezza Cucinelli and Fabiana de Araujo Pinto, for the laboratorial support.
