
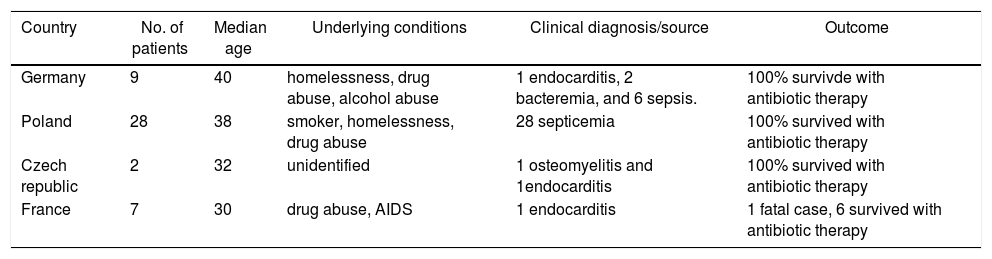
Invasive diseases caused by Corynebacterium diphtheria occur very rarely and when they involve Corynebacterium diphtheria nontoxigenic strains, they can cause atypical course of the disease. In the last years several articles from Poland,1,2 Germany,3 Czech Republic,4 and France5 have reported invasive diseases caused by Corynebacterium diphtheria nontoxigenic strains suggesting a spread of these pathogens in Western Europe (Table 1).
Reported cases of Corynebacterium diphtheriae nontoxigenic strain septicemia in Europe.
| Country | No. of patients | Median age | Underlying conditions | Clinical diagnosis/source | Outcome |
|---|---|---|---|---|---|
| Germany | 9 | 40 | homelessness, drug abuse, alcohol abuse | 1 endocarditis, 2 bacteremia, and 6 sepsis. | 100% survivde with antibiotic therapy |
| Poland | 28 | 38 | smoker, homelessness, drug abuse | 28 septicemia | 100% survived with antibiotic therapy |
| Czech republic | 2 | 32 | unidentified | 1 osteomyelitis and 1endocarditis | 100% survived with antibiotic therapy |
| France | 7 | 30 | drug abuse, AIDS | 1 endocarditis | 1 fatal case, 6 survived with antibiotic therapy |
Herein we present a 30-year-old male soccer player with septicemia associated with a diagnosis of osteomyelitis of the pubic symphysis. The agent, Corynebacterium diphtheriae nontoxigenic strain, biotype mitis, was identified by serial blood cultures.
Previously healthy, the man was admitted to the Emergency Department of Infectious Diseases of the Hospital na Bulovce (Nemocnice na Bulovce) in Prague with fever, headache and groin pain. There was no history of recent tick bites, exposures to sick contacts or animal exposure, illicit drug use, or travel outside Czech Republic. On physical examination, his temperature was 38.1 °C, blood pressure 98/50, heart rate 118, and he manifested lower abdominal tenderness and pain. There were no further abnormal findings. Laboratory examination showed elevated inflammatory parameters, C reactive protein 159 mg/l (normal value <8 mg/l). The white blood count was 14,200 cells/mm3 with no shift to the left, thrombocytopenia 80 × 109/μL (normal value range 150.000–450.000 109/μL), and creatinine 140 mg/L (normal value range 50–90 mg/L). Urine analysis was normal and culture negative; a plain abdominal radiograph was normal.
Clinical re-evaluation showed localized tenderness in the pubic area. In a more detailed history, the patient reported that for the last year, he had trained extensively as a soccer player (at least six times a week). After exercising he experienced pain in the pubic region and stiffness for two days. A contrast-enhanced abdominal and pelvic computed tomography was performed and identified bony destruction on the margins of the symphysis pubis, suggesting osteitis pubis. The diagnosis of symphysis pubis osteomyelitis was then confirmed by magnetic resonance imaging (MRI) of the pubic region.
Four blood samples were drawn during the first day of hospitalization for microbiological evaluation, and empirical intravenous antibiotic therapy (co-amoxicillin and gentamicin) was started. All four blood cultures (BD BACTECTM FX [Becton Dickinson] bottles) showed a rich growth of Gram-positive rods, identified as Corynebacterium diphtheria sensitive to penicillin, oxacillin, ampicillin, cefalotin, erythromycin, clindamycin, cotrimoxazole, tetracycline, and ofloxacin. The isolated strain was confirmed by the National Reference Laboratory for Pertussis and Diphtheria of the National Institute of Public Health, Prague.
The strain was identified as C. diphtheriae biotype mitis, nontoxigenic strain. The strain was characterized by biochemical method (API Coryne, BioMérieux, France) and by mass spectrometry (MALDI TOF, Bruker Daltonics, USA). Diphtheria tox gene was screened by real-time PCR.
Upon results of the antibiogram, antibiotic de-escalation to G-penicillin was adopted. Fever and inflammatory blood markers normalized after one week of intravenous antibiotic treatment, but the severe pain was still present, which indicated surgical revision and debridement of the purulent cavity of os pubis. Histological examination of biopsy specimens showed bony destruction, osteolysis and fibrotic zones with clusters of histiocytes with signs of acute osteomyelitis, cultivation of excochleated bone tissue were sterile.
Postoperative recovery went without any complications and the patient was discharged home after 30 days of hospitalization. Antibiotic treatment was continued orally for three weeks (cotrimoxazole). The patient did well after surgery and had no complications. He was then seen in the clinic after one month, two months, four months, and six months and magnetic resonance imaging (MRI) assessments were performed each time. So far, these measures have caused him a noticeable relief and he has since then returned to his daily routines despite some occasional pain.
According to data from medical databases, this is the second report of septicemia caused by C. diphtheriae nontoxigenic strain in an immunocompetent adult in Czech Republic.
C. diphtheriae nontoxigenic strain can produce atypical manifestations of a disease and it is a rare cause of sepsis in immunocompetent patients because of high rate of immunization coverage against diphtheria, as is the case in the Czech Republic. It is relatively rare in immunocompetent patients, as well as in geographic areas with no cases reported of diphtheria and other C. diphtheriae infections. Cases of septicemia by C. diphtheria nontoxigenic strain were however reported in other European countries, suggesting that nontoxigenic Corynebacterium diphteriae strains are sufficiently pathogenic to cause disease. The diagnosis of our patient was surprising as he does not belong to any of the mentioned typical risk groups (gynecologic or urologic surgery, pelvic malignancy, intravenous drug use, and immunodeficiency) and no connection between bacteremia, skin lesions or other risk factors was found. The bacterium was reported to have developed resistance to commonly used antibiotics, but fortunately, in our case, it showed good sensitivity to these antibiotics.
The pathogenesis of infection caused by nontoxigenic Corynebacterium diphteriae is unknown and requires investigation. We know that current vaccine against diphtheria contains the toxoid so it protects only against the toxigenicity but not against the invasiveness of C. diphtheria. It is thus important to show that infections connected with C. diphtheria can occur in an immunized population. It is possible that the high rate of immunization with diphtheria toxoid may place selective pressure on the microorganism to develop other pathogenicity factors. For this reason, we must consider this bacterium as a potential pathogen in immunized populations.
ConsentWritten informed consent was obtained from the patient for publication of this case report.
Conflicts of interestThe authors declare no conflicts of interest.
The authors would like to thank Ms Kamila Etchegoyen Rosolová, PhD Head of Center for Academic Writing in Prague, for the revision of the manuscript.
