
In 1937, the foundation year of the Brazilian Institute for Tuberculosis Research, three questions persisted in the researchers’ mind: “What is the real value of BCG? How to solve the problem of the chest register of large communities? When will we have a specific drug for the treatment of tuberculosis?” Along with this line of thought, the author presents a list of the Institute's main contributions, by pointing out the following topics: different diagnoses between pulmonary tuberculosis and pulmonary schistosomiasis; innocuity of iodine salts in pulmonary tuberculosis; relative value of Weltmann and Takata-Ara's reactions, and of blood and lipase rates in bacillosis; the value of the bacteriologic diagnosis (method of precipitation, standardization of drug sensitivity tests; identification of non-pathogenetic germs not only in the sputum but also in gastric Broncho-Alveolar Lavage, playing an important role in the infection tropics; probable protective role of BCG in tuberculin positive individuals; increase in awareness of the value of tuberculin; comparative studies of several types of tuberculin; clinical and epidemiological importance of nontoxic drugs; tuberculin surveys in Salvador and Feira de Santana cities; proposed classification of clinical forms of pulmonary tuberculosis; increase in the value of selective miniature chest radiography; standardization of radiological shadows; and tests on the therapeutic value of the drugs. To SILVEIRA, IBIT'S contribution can be summarized in eight points: importance of bacteriology in the diagnosis and therapeutic procedures; increase in the value of tuberculin tests; selective miniature chest radiography; possibility of replacing the hospital by an ambulatory care center; BCG vaccination; wide and general indispensability of a well-done and well-balanced therapeutic scheme; simplified treatment; progressive shortening of the treatment program; no over optimism about the first victories in the bacilli therapy.
In 1937, the year of establishment of IBIT, three questions persisted in the investigators’ minds: (1) What is the true use for the BCG? (2) How to solve the problem of thoracic investigation in large crowds? (3) How to get a specific medication for tuberculosis? The IBIT during its first fifty years, tried to answer these questions.
Tuberculosis and co-morbiditiesBelonging to a tropical country, the Institute began studying the correlation of tuberculosis with ascariasis,1 malaria,2 filariasis3 and schistosomiasis.4–9 About schistosomiasis, Silveira elucidated some clinical and pathologic features. Silveira demonstrated that, in its lung location, it causes several vascular disorders2 and a pneumonitis image. The fact was corroborated by Shaw and Ghareb in Egypt, and Alves Meira in Sao Paulo.9 Knipping, included the “Silveira's pulmonary bilharziosis”, while discussing the cor pulmonale risk factors.
Development of therapy for tuberculosisBefore the modern armamentarium of chemotherapy, the IBIT tested the importance of some substances although without bacteriostatic or bactericidal effects as an adjunct of therapy as no effective drugs were available at that moment. We cite as an example the work of Silveira and Silveira and Costa on salts of calcium, iodine,10 copper and gold.11,12 Silveira said: “based on carefully performed clinical histories with documented radiological and laboratory tests, we have been able to heal many people, as denounced in some published papers”.13
From the tentative chemotherapy insecure IBIT worked on the collapsotherapy and artificial pneumothorax, methods of use in Bahia, at that time. Codes and Sandoval14 began the practice of phrenicectomy, Macedo Costa devoted himself to the study of pleural adhesions,15 and Bridges16 embarked on the thoracoplasty, Cardoso and Góes17 in the pulmonary resection.
Rist et al. studied clinically 2nd line drugs in collaboration research protocols. These studies made it possible for IBIT to use experimentally several drugs (isoxil, ciclocerina, ethionamide, pyrazinamide, ethambutol and rifampicin) and its application in economic simplified schemes and combinations.
This paper from Silveira et al.18 on intermittent chemotherapy of tuberculosis is noteworthy. These authors, based on an experimental model of GRUMBACH investigated: (1) the importance of a triple daily regimen for one month, with the combination Isoniazid (INH), Streptomycin and Ethambutol (EMB); (2) this previous regimen forwarded by the intermittent use of the combination of INH-EMB, three times per week, using double and normal dosage, and (3) the intermittent action of INH+EMB three times per week, daily for one month without streptomycin. In 1968, the authors were encouraged by the results with the combination EMB+DAT+Ka in patients with persistent positive cavitary lesions, some of them with history of collapsotherapy, resistant to 1st and 2nd line drugs, considered irrecoverable after prolonged hospitalization (average of four years), so Silveira, recommended this intervention to diminish prolonged hospitalizations.19
Some of the pharmaceutical companies have asked the IBIT to test new proposed drugs. Interested in a substance able to replace the para-amino-salicylic (PAS), Silveira et al.20 used a thiurea derivative, known for its tuberculostatic action [diisoamylhydroxythiocarbanilide (Isoxyl)].21 They used the product in three patients with previous history of prolonged treatment, resistant to traditional drugs. Two patients did not respond but the third one the smear became negative. However, this latter case had undergone thoracoplasty during treatment and the results were considered doubtful, the drug however was considered with good tolerance.
Aiming to determine the power of this tuberculostatic drug, the authors selected four patients hospitalized in the Thorax Hospital (presently Hospital Santo Amaro) and twelve from the of IBIT outpatient clinic. Of the latter, one died early during the trial, one died during treatment, and six left the trial after the first prescription. Only eight patients completed the treatment. In all cases, after a sometime, the drug under test (Isoxyl) was required to be associated with other drugs, since, despite producing some effect, the Isoxyl did not cure the disease. The conclusion was that the drug subjected to experimental conditions was completely unfavorable for patients with long history of treatment with very advanced lung processes and releasing resistant bacilli to all classic drugs. In a single patient, previously untreated, the result was much better, not achieving a complete success because the drug was first used alone in doses considered subsequently insufficient. No intolerance was registered for any case. Conclusions were firstly, it was clear that the result is more effective in naïve patients. Secondly, the use of DAT demonstrates that the drug was unable to cure by using alone. Thirdly, association with strong tuberculostatic drugs seems to reinforce the action of the drug.
Tuberculosis diagnosis trialsFrom early 30s to 40s IBIT developed research on blood glucose reactions,22 while the value of Welmann23,24 and Takata-Arada25 reactions conducted research on precipitation in double diffusion Agar,26 hematic levels,27 and erythrocyte sedimentation rate24 in patients with pulmonary tuberculosis. Darzins contributed greatly to the success of these findings.28 Thanks to Darzins IBIT developed the method of agitation / precipitation,29 and standardized the drug sensitivity tests (at a time when these were virtually unknown in Brazil), where he also discovered several species of the genus Mycobacterium, and newly described the Mycobacterium gyae30 and other nonpathogenic bacteria isolated from sputum, bronchial and gastric lavages.31
Other foreign scientists and technicians who worked in IBIT contributed enormously in the basis of the institution to greater awareness of the disease. Among these scientists we can highlight Canetti (France), Pantzer (Romania), Cetrangolo (Argentina), Reutgen (Germany), Bravo (Spain), Gossner (Germany), Lorian (United States) and Hilscher (Germany), and Rist et al. Among the technicians it can be mentioned that Elizabeth Gheno, who contributed to the organization of the Department of Pathology and Hans Geissler who contributed to the creation and organization of the Department of Scientific Documentation. Canetti established standards for the resistance evaluation of M. tuberculosis to antituberculosis drugs. To him is credited the knowledge of the bacterial flora of tuberculous lesions and the basic conditions for the application of antituberculosis chemotherapy in Brazil. To Canetti, Grosset and Grumbach we owe the proportional sensitivity test and IBIT was the first to use this test in northern and northeastern Brazil.32
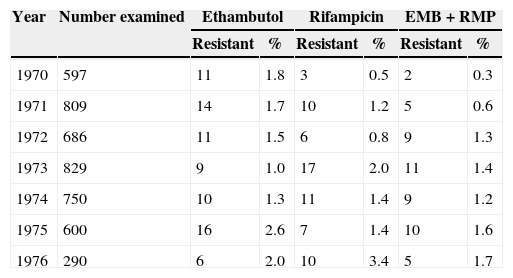
Due to its high concept at that time in performing drug sensitivity tests, the IBIT was also looked upon to perform surveys of industrial interest. It was the case sulfate-reducing bacteria isolation and the bactericidal action of certain chemicals by such bacteria, research of interest in this case by Petróleo Brasileiro SA (PETROBRAS).33 In many opportunities IBIT was asked to clarify doubts and clarify issues related to diagnosis, therapy and prophylaxis of tuberculosis as well as opine on epidemiological issues. An example of this is the survey on the resistance of M. tuberculosis against EMB and RMP, during the years of 1970 to 1976 (Table 1).
Prevalence of resistance to ethambutol and rifampicin of Mycobacterium tuberculosis isolates from 1970 to 1976 at the Instituto Brasileiro para a Investigação da Tuberculose.
| Year | Number examined | Ethambutol | Rifampicin | EMB+RMP | |||
|---|---|---|---|---|---|---|---|
| Resistant | % | Resistant | % | Resistant | % | ||
| 1970 | 597 | 11 | 1.8 | 3 | 0.5 | 2 | 0.3 |
| 1971 | 809 | 14 | 1.7 | 10 | 1.2 | 5 | 0.6 |
| 1972 | 686 | 11 | 1.5 | 6 | 0.8 | 9 | 1.3 |
| 1973 | 829 | 9 | 1.0 | 17 | 2.0 | 11 | 1.4 |
| 1974 | 750 | 10 | 1.3 | 11 | 1.4 | 9 | 1.2 |
| 1975 | 600 | 16 | 2.6 | 7 | 1.4 | 10 | 1.6 |
| 1976 | 290 | 6 | 2.0 | 10 | 3.4 | 5 | 1.7 |
BEM, ethambutol; RMP, rifampicin.
The papers of Silveira34–38 and Silveira and Medeiros39–42 on the protective power of BCG in allergic patients are of great importance. The research aimed to answer the following questions: (1) What should be done with the high percentage of infected individuals without active tuberculous lesion, which are forced to live with smear positive tuberculosis? (2) What should be done with the family members of a patient with tuberculosis, when its isolation is impossible and a fatal infection is present in an environment with several exposed? In addition, for those infected, what should be done? Silveira and Medeiros analyzed the results obtained with the observation of 57 allergic patients, vaccinated with BCG orally in doses ranging from 0.10 to 0.50g. The research led to the following conclusions: (1) BCG is completely innocuous for individuals already infected, even when living in an environment with high probability of infection and reinfection. (2) In addition to innocuous, the prospect, in such individuals, of their protective role. (3) After repeated BCG vaccination, there is a possible increase of the immunity of primo-infected. (4) Days after the use of the oral vaccine, there is exaltation of cutaneous sensitivity to tuberculin, followed by pronounced attenuation and even complete extinction of allergy. (5) The loss of allergy seems to depend on genetic component. The BCG was beneficial not only for the newborns but also for those who have not been contaminated by M. tuberculosis, and even in those already infected, “allergic”. BCG may have shown appreciable protective power against successive re-infections. The data obtained were limited in time and space, and if the application by mass vaccination of allergic is not authorized, it requires that these investigations be repeated on a larger scale because, proven conclusively the existence of the protective power of the BCG for allergy sufferers, will have taken a step toward the tuberculosis prophylaxis, especially in countries with a high incidence rate of this disease, where there is a high percentage of allergic exposed to infection.
Tuberculin studiesIn particular BCG and tuberculin diagnosis, owe much to the IBIT studies of Silveira, Durval, Freitas and Medeiros.43–45 Confirming previous observation,46 Silveira said the fact that large and repeated doses of BCG do not result positive response in some newborns, even when employing the dermal one, seems to be linked to a familial predisposition.47 Silveira vaccinated those with positive tuberculin, the sick and apparently healthy with good results; “with this, the IBIT, Stela Medeiros and I, we entered the École Brésilienne of BCG, so expected, especially for the French professors and researchers Drs. Max Fourestier and Gernez Rieux” wrote Silveira once. IBIT removed several “dogmas”47 that prevented the wide application of BCG: the obsession of allergy, the failure of the oral method, the dangers of vaccination of perennial allergic and immunizing the primary infection. The scope of this achievement is of utmost importance for developing countries, where there are masses of people uneducated, lack of hospital beds and lack of qualified technicians.
Medeiros42 published an important work on exposure to infection, infection in children, epidemiological surveys, comparison between different known tuberculin preparations, including raw and purified ones, and disappearance of reaction in certain circumstances. The IBIT conducted a comparative study of tuberculin BCG2 and BCG3 (provided by Assis) and tuberculin purified from Germany, Denmark and France. “If, at first glance, the tuberculin purified, should be preferred – Silveira says – and in fact increasingly – we must not forget that the old tuberculin of Koch (especially if prepared in synthetic media) continues to offer regularity good results and an accuracy of specificity that cannot be ignored”. The investigations carried out in IBIT demonstrated that the use of tuberculin in a dilution of 1/10 (10mg raw tuberculin), plus weaker dilutions, would discover about 10% more allergic. The verification of the Saye-Willis phenomenon, caused by mouth, adds 12% positivity. “Testing with weaker tuberculin concentrations (1/1000 or 1/100), as has been widely practiced, is missing many already infected as false non-allergic and therefore true allergy ones have been widely vaccinated”.
Durval44 showed that among those who lost their tuberculin allergy there is predominance of young individuals less than 20 years of age. Contrary to the widespread belief, Silveira noted that this loss is made in similar proportions in both males and females, being more pronounced when administering the BCG. Regarding ethnicity, both in the vaccinated as non vaccinated, the loss among African descents was much more pronounced (50%). When the loss of allergy was more difficult when initial allergic reactivity was greater. This tendency was greater in those vaccinated with BCG, and in those this figure could raise to 100% of allergy loss. Rosemberg and Silveira48,49 demonstrated that, contrary to what was sustained, the repeated use of BCG does not cause allergy. Rather, it attenuates. This desensitization is very sharp and can reach total extinction. This loss of allergy is beneficial or harmful to the patient? Trying to find the answer, Silveira,50 after two years of accurate observation, found in 37 vaccinated, only 3 patients with nonspecific pulmonary processes, so 91% of cases without any clinical signs or radiological or laboratory abnormalities. Among the controls, the percentage was slightly lower, i.e., 88%. The conclusion was the recognition of the existence of re-infection in individuals being labeled as a primary infection. In the opinion of Silveira the existence of primary forms of infection in adults should be rare and its labeling much more cautious.
In 1939, under the direction of Silveira,51 a survey was conducted in the city of Salvador tuberculin in boarding schools for poor children and Penitentiary (largely inmates in the state, young adults). Hygiene conditions were equivalent, as well as food and labor regime. Three dilutions (1/25,000, 1/100 and 1/10) were used. Hyper-reactors were considered as those reactors to the first dilution; medium-reactor those positive to the second dilution; hypo-ergics, as those positive only to the third dilution. ASSIS demonstrated the existence of individuals who maintained their allergy below the ordinary (infra-tuberculinic allergy of Assis),52 which makes it necessary to awaken the allergy with a dose of BCG to repeat after the intradermal to 1/10. Strictly speaking, only people who respond negatively should be considered not allergic.
The purpose of tuberculin survey was to discover those not allergic, so targeted to BCG vaccination. In Brazil, first Assis52,53 then Silveira38 and Silveira and Medeiros41 proved that BCG does not affect the allergic and therefore recommended not “molesting” the individuals with the completion of several tests. We vaccinate indifferently performing “mass vaccination”. Race; influence of several physiological states such as pregnancy, hormonal and nutritional factors; and even geographic variations may modify the allergic state. Even saprophytic bacilli can cause positive reactions. Such factors exist, are rare and have no influence on the tuberculin overall status, and its epidemiological interpretation. Two thousand one hundred thirty-five people were tested, of these, 87.6% were reactors and 12.4% non-reactors. Of those non-allergic, 26.1% were falsely non-allergic. The percentage of reactors increased rapidly after 5 years of age. The peak was observed in ages from 15 to 20, and then a decline was observed with advancing age. That has not stopped people with advanced age to present strong reactions. Between 80 and 90 years of age, 33 people were found positive, of which 14 were hyper-ergics, 18 normal-ergics and only one hypo-ergic. The reactions were stronger in African descents. Among the false reactors predominant white race (21 white and 8 African descents). Among men, there was a predominance of those hyper-ergics and among women the predominance were normal respoinseve or hypo-ergics.
Studies on radiology of tuberculosisIn Brazil, the forms of primary infection and re-infection are common. The forms of re-infection are rare and exceptional circumstances and when they arise, they often replicate from the primary infection, so it is not always easy to distinguish. Santos54,55 has contributed to many aspects of radiological investigation in IBIT.
The work of Costa56 about radiological topography is noteworthy: “Taking as its point of reference 6th and 9th ribs and drawing two horizontal lines across the the chest, I have divided the lung fields in three areas: upper, middle and lower. These three zones are in turn subdivided into two regions – internal and external – on a vertical line starting from the middle half of the clavicle of the diaphragm homologous”. Shortly after, Silveira had proposed systematization of pleuropulmonary images based on three modalities: images condensation (with the types miliary, nodular, nummular, linceolar, linear, fascicular and reticular), refractive images (with the types emphysema and pneumo) and mixed images (with spongiloid types, ring and air-fluid). Of unquestionable value to the time of its publication is the experience of Costa tomography of lung. Costa recommended the necessity of stratigraphy: (1) In search of the tuberculosis with cavities (outline contour, volume and depth). (2) The elucidation of the possible existence of cavity before thickening, or rather of a pleural effusion. (3) In choosing the best surgical option, considering the extent of resection of the ribs and number of operative sessions, and (4) control of the therapeutic result, face closure or not the cavity.57
Among the reasons that led to the abandonment of roentgenphotography58,59 in epidemiological surveys, was the finding of potential doubtful shadows, outside the conditions of an open tuberculosis, easy disclosure by bacteriological. In 1951, Silveira,41 in the 5th National Congress of Tuberculosis, presented a proposal to standardize the patients diagnosis with thoracic shadow, and their medical and social significance.
Studies on sputum smear baciloscopyOliva60 comparing culture results with those obtained by direct microscopy concluded that in about 30% of cases the culture is positive, while the smear is negative. The same author used the antigen for testing the reaction of precipitation in double diffusion in agar.61 Machado,26 using this antigen in 43 patients with tuberculosis obtained 18 positive results (44%), 11 undetermined and 13 negative ones. When the discordant results were tested again, 60% positivity was achieved.
The appreciation of the bacteriological examinations was an important contribution. Silveira37 summarizes this contribution on five items: (1) Suppression of strong acids and alkalis in the preparation of material for culture and inoculation. (2) Isolation of mycobacteria non-pathogenic to guinea pigs with morphological and cultural properties identical to M. tuberculosis. (3) Possibility of higher frequency non-pathogenic bacteria in the tropics. (4) Attenuation of germs by chemotherapy, or by the elimination of BCG (tuberculin-positive individuals). (5) The need for a detailed study on the frequency and nature of non-pathogenic germs, not only to improve the quality of bacteriological diagnosis but also to know more accurately the biology of M. tuberculosis.
ConclusionWe quote Silveira who summarized the participation of IBIT in eight points: (1) the fundamental importance of bacteriology in the diagnosis and therapeutic management of the patient with tuberculosis, (2) enhancement of the tuberculin test for perfecting the knowledge of the immune status of the patient; (3) selective roentgenphotography instead of widespread use of the Abreugraphy (4) ability to replace the treatment from hospital based to out-patient clinic, and the new results are rich and secure, (5) extensive and widespread vaccination without prior tuberculin tests, (6) Indispensability of a therapeutic schema well-conducted and well-balanced, based on carefully selected drugs; (7) progressive shortening of the treatment program, and (8) complete rejection of victory without new resources and means to combat the disease. “Such results”, he said, “have not given us, is truth, enough originality to profoundly alter the evolution of scientific thought. We were victims of our poverty, without adequate human resources and equipment, working on our own, with pour and uncertain support of official aid, never managed to create the adequate technical and functional means indispensable to mount the program dreamed”.
Conflicts of interestThe author has no conflicts of interest to declare.
