





World Health Organization estimated that people with diabetes (DM) are at 2–3 times higher risk for tuberculosis (TB). Studies have shown that DM not only increases the risk of active TB, but also puts co-affected persons at increased risk of poor outcomes.
ObjectivesTo determine the protective effect of metformin against TB in DM patients and also, to investigate the relationship between poor glycemic control and TB.
MethodsA case–control study was conducted over 8 months, where cases and controls were selected based on the inclusion and exclusion criteria of the study. The diabetics diagnosed with TB were selected as study group (SG=152) and without TB were as control group (CG=299). Exposure status of metformin in both groups were analyzed.
ResultsThe mean (SD) age of both CG and SG were 55.54±11.82 and 52.80±11.75, respectively. Majority of the subjects in the study were males. The mean hospital stay of SG and CG were 7 days and 6 days, respectively. Poor glycemic control (HbA1c>8) observed in SG (51.7%) vs CG (31.4%). HbA1c value <7 is associated protective factor for TB occurrence [OR=0.52 (95% CI 0.29–0.93)]. The protective effect of metformin against TB was 3.9-fold in diabetics (OR=0.256, 0.16–0.40).
ConclusionPoor glycemic control among diabetics is a risk factor for TB occurrence. The result shows metformin use is a protective agent against TB infection in diabetics. Hence, incorporation of metformin into standard clinical care would offer a therapeutic option for the prevention of TB.
Tuberculosis (TB) is one of the most common infectious diseases causing morbidity and mortality worldwide. Each year, approximately 9.6 million new cases and 1.5 million deaths occur due to TB.1,2 India has the highest burden of TB.3 More than 95% of TB deaths happen in resource-poor low and middle income countries. Persons with compromised immune states, such as HIV infection, diabetes, tobacco use, and malnutrition are at a greater risk of progressing from latent to active TB.2 It is possible that in areas of high prevalence of diabetes, the impact of the DM epidemic on tuberculosis could be as great as that of HIV.
Globally, around 15% of TB cases are estimated to be attributable to DM.4 The escalation of diabetes prevalence in TB-endemic regions may adversely affect tuberculosis control. The current Indian diabetes scenario could lead to resurgence of TB in endemic regions, especially in urban areas.5 Diabetic patients with TB have negative treatment outcomes such as delay in sputum culture conversion, increased risk of death during treatment, and TB relapse after successful anti-tubercular treatment regimen.2 Diabetic TB patients suffer from higher mortality (7.5%) compared to patients with either TB (1%) or DM (2%) alone.6 A study from Kerala (Southernmost state of India) demonstrated that diabetics with drug sensitive TB have greater probability of failing first line TB treatment as compared to those without DM.7,8
Diabetes is associated with diminished innate and adaptive immune responses which are essential to combat the intracellular proliferation of Mycobacterium tuberculosis (M. tb). Host cell recognition is diminished in diabetics, resulting in the decline of immune response, which render diabetics more susceptible to bacterial infections. Control of TB comprises various strategies such as case treatment, preventive therapy, and vaccination with BCG.9 TB prevention and control could be further improved by interventions that counter known risk elements of TB such as diabetes, immune compromise in conditions like HIV.
Currently, there are a number of difficulties in developing new drugs with potential anti-TB effects, especially with therapeutic and prophylactic efficacy against dormant M. tb organisms. The current anti-tubercular therapy is long drawn and is associated with drug toxicity and heightened multi-drug resistance. Therapeutic modulation of host cell responses that enhances pathogen eradication is being suggested as a new paradigm in drug discovery. These ‘host-targeted’ therapeutic strategies are less likely to provoke microbial resistance than targeting pathogens with conventional drugs.
Innate antimicrobial arsenal of the host cell includes reactive oxygen species (ROS) and reactive nitrogen species (RNS), in addition to the phagosomal machinery or autophagy. Autophagy is controlled by mammalian target of rapamycin (mTOR) complex-1 and adenosine monophosphate activated protein kinase (AMPK).10,11 Singhal et al. demonstrated that AMPK-activation by metformin inhibits intracellular growth of M. tb, restricting disease immunopathology, and enhancing the efficacy of conventional anti-TB drugs. Singhal's data suggest that both protective immunity and pathological immunity can be independently modulated by metformin during M. tb infection by enhancing M. tb-specific host immunity, reducing inflammation, promoting disease resolution, and improving treatment outcomes. At the cellular level, metformin differentially affects immune response and inflammation through different mechanisms. The protective effect is mediated by increased host cell production of mROS and increased acidification of mycobacteriod phagosome. Actually, mROS produced upon mitochondrial recruitment to phagosomes is instrumental in killing of intracellular bacteria by macrophages. The anti-inflammatory effect is mediated by activation of AMPK. Metformin also promotes the expansion of M. tb specific IFN-γ-secreting CD8+ T cells in uninfected mice indicating that metformin has an impact on the lung immune cells independently of current infections. These effects are consistent with metformin-induced expansion of CD8+ memory T cells, another known consequence of AMPK activation. Both CD4+ and cytotoxic T cells are key to controlling primary M. tb infection in human subjects. Studies by Singhal et al. have also shown an increase in M. tb-specific T cells in metformin treated diabetic patients with latent TB. Metformin therapy combined with standard TB treatment regimens has demonstrated beneficial clinical outcomes in active TB.
We hypothesize that metformin, via AMPK-activation, boosts host immunity and thereby protect DM patients from TB. As metformin is the most frequently prescribed oral anti-diabetic in clinical practice, and since its mechanism of action, including AMPK activation, is well known, a comprehensive preventive strategy of TB in DM should mandate the use of metformin in all diabetics unless contraindicated.
Materials and methodsThis case–control study was conducted in a tertiary care hospital in South-India (Kasturba Hospital (KH), Manipal) for a period of eight months (August 2015 to March 2016). Data of patients admitted during Jan 2011 to Dec 2015 were obtained retrospectively from the Medical Records Department of the hospital. Subjects were identified based on ICD-10 coding for disease classification (Diabetes without complications: E11.9; tuberculosis: A15–A19). Study subjects were divided into study group (SG: 152) and control group (CG: 299). SG consisted of diabetics diagnosed with TB and CG had diabetics without TB. The ratio between case and control was kept as 1:2. The inclusion criteria was age ≥40 years. Patient's anti-diabetic medications (metformin or other anti-diabetics or its combinations) usage status were noted.
We used computerized records for identification of case and controls, assessment of comorbidities, and ascertainment of outcome. Control data were collected from discharge summary and identified newly detected diabetes patients with no history of TB, meeting inclusion criteria. Patients diagnosed with DM before 2011, below 40 years, with tuberculosis were excluded from control group. Both case and control data were from the same hospital, with similar exposure status and at risk of developing similar outcome.
The CRF captured demographic data (age, gender, weight, height, BMI, occupation, and social habits) and clinical details (chief complaints on admission, past medical and medication history, case category, comorbid condition, diagnosis, allergy status, laboratory parameters, treatment, prognosis, discharge medication). Data were collected for population exposed to metformin and non-metformin, i.e. other oral hypoglycemic agents, OHA's (sulfonylureas, alpha glycosidase inhibitors, thiazolidinedione, meglitinides or insulin) or combinations.
Sample sizeClinical significance in the incidence rates between SG and CG was fixed at 5% with 80% power and 5% level of significance. As the ratio of SG:CG was fixed at 1:2, the minimum number of subjects required in SG and CG were determined to be 150 and 300, respectively. Therefore, a total sample size of 450 subjects were included in the study.
Statistical analysisNumber and proportion of patients with metformin in the TB case group is the main outcome for the analysis. Results were reported as rates & percentages for categorical variables, and mean & standard deviation for continuous variables. For univariate analysis, Chi-square was used. For the intervention measures, the absolute risk reductions and the number needed to treat to prevent TB in one person was calculated. p-Value <0.05 was taken as statistically significant.
Ethical clearanceEthical clearance for study was obtained from Institutional Ethics Committee of Kasturba Hospital, Manipal (IEC 430/2015).
ResultsStudy populationWe identified a total of 451 cases (Control, CG: 299 and Case, SG: 152) which included 299 controls, 128 diabetics not on metformin and 171 diabetics on metformin. Among the 152 cases, 111 were not on metformin and remaining 38 were on metformin. General characteristics of study population are summarized in Table 1.
General characteristics of study population.
| Parameters | Cases (N=152) | Controls (N=299) |
|---|---|---|
| Age in years (mean±S.D.) | 52.8±11.7 | 55.5±11.8 |
| Gender (%) | ||
| Male | 124 (82) | 194 (65) |
| Female | 27 (18) | 105 (35) |
| Duration of hospitalization (days) [median (range)] | 7.0 (5.0,10.0) | 6.0 (4.0,8.0) |
| Number of hospitalization [median (range)] | 1.0 (1.0,2.0) | 1.0 (1.0,2.0) |
| BMI (mean±SD) (kg/m2) | 21.2±3.7 | 25.8±15.7 |
| Symptoms on admission [No (%)] | ||
| Cough | 100 (66.2) | 38 (12.5) |
| Fever | 81 (53.6) | 29 (9.7) |
| Weight loss | 17 (11.3) | 6.0 (2.0) |
| Breathlessness | 15 (9.9) | 15.0 (5.0) |
| Fatigue | 17 (11.3) | 11.0 (3.7) |
| HbA1c(%) [median±IQR] | 9.3 (7.5,11.6) | 7.9 (6.8,10.7) |
| FBS (mg/dl) [median±IQR] | 178 (124,243) | 163 (125,234) |
Among the 299 CG, 194 (64.9%) were males and 105 (35.1%) were females. In SG, 120 (79.5%) were males and remaining of 24 (15.9%) were females. The mean (SD) age of both CG and SG were 55.54±11.82 and 52.80±11.75, respectively. We found that in both SG and CG, poor glycemic control (i.e. HbA1c>8.0) was seen in 51.7% and 31.4% of patients, respectively. Similarly, FBS>100mg/dl was seen in 87.4% of SG and 57.9% of CG [Table 2]. Thirty-eight (25.5%) people in the SG and 171 (57.1%) in the CG were using metformin. Moreover, a significant proportion were not prescribed metformin in both SG (n=111; 74.5%) and CG (n=128; 42.8%) [Table 3].
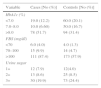
Glycemic status in the study groups.
| Variable | Cases [No (%)] | Controls [No (%)] |
|---|---|---|
| HbA1c (%) | ||
| <7.0 | 19.0 (12.2) | 60.0 (20.1) |
| 7.0–8.0 | 10.0 (6.60) | 50.0 (16.7) |
| >8.0 | 78 (51.7) | 94 (31.4) |
| FBS (mg/dl) | ||
| <70 | 6.0 (4.0) | 4.0 (1.3) |
| 70–100 | 15 (9.9) | 14 (4.7) |
| >100 | 111 (87.4) | 173 (57.9) |
| Urine sugar | ||
| 1+ | 12 (7.9) | 12(4.0) |
| 2+ | 13 (8.6) | 25 (8.5) |
| 3+ | 30 (19.9) | 73 (24.4) |
Metformin usage patterns in the study groups.
| Exposure status | Study outcome | Total | Statistical tests | |
|---|---|---|---|---|
| Case [No (%)] | Control [No (%)] | |||
| Present (metformin) | 38 (18.2) | 171 (81.8) | 209 (100) | Chi2=40.12; p=0.00 OR=0.256 (0.16, 0.40) |
| Absent (non-metformin) | 111 (46.4) | 128 (53.6) | 239 (100) | |
| Total | 149 (33.3) | 299 (66.7) | 448 (100) | |
Use of metformin at any time was significantly associated with reduced risk of TB. Odds ratio<1 shows that metformin is protective against TB by a factor of 3.9. We did not find any dose dependent protection in metformin users. No difference was found between those on 1000mg metformin, (27.3%) and on 500mg (25.7%) for development of TB. Dose of metformin does not seem to affect the protective outcome of metformin against TB infection (OR=0.92; Chi2=0.05; p=0.82).
According to our study results, HbA1c value less than 7 was found to be protective against TB occurrence (OR<1), showing that poor glycemic control is associated with increased risk of TB infections [Table 4].
DiscussionMales outnumbered females in both CG and SG by 64.0% and 29.8%, respectively. A similar trend in male dominance was observed in other studies by Dobler et al.,12 and Feza et al.13 TB incidence was highest in diabetics aged 51–60 years (n=47) in this study. According to Dobler et al.,12 the majority of TB in DM patients was observed in age group of 55–74 years. The reason could be because metabolic disorders can even at a younger age in Indians compared to Westerners.14,15 Our inclusion criteria, had subjects more than 40 years. TB incidence was not age-dependent; 51–60 years (30.9%) and 41–50 years (26.3%). However, the incidence of TB was lower in elders 61–70 years (n=24, 15.8%) and above 70 years (n=12, 7.9%).
We found that smoking and low income were significantly associated with treatment failure of TB, which is in agreement with another study by Tachfouti et al.16 Low socioeconomic status indicators such as overcrowding, illiteracy, low wages and unemployment were associated with increased risk for TB as well as poor medication adherence.17
We observed that the majority of TB patients did not have any significant family history (84.8%). However, 11.9% cases had family history of diabetes but very low incidence (2.6%) of family history of TB. Due to incomplete medical records and poor family history documentation by physicians, family history data were missing in most of our study population. Most frequently observed symptoms in SG were cough (66.2%), fever (53.6%), weight loss (11.3%), fatigue (11.3%) and breathlessness (9.9%). The majority of SG had a poor control of glycemic levels, with HbA1c>8% (51.7%) and FBS>100mg/dl (87.4%). A systematic review by Christie et al. in 2010 demonstrated higher incidence of hyperglycemia in TB, ranging from 1.9 to 35%, possibly because of chronic inflammation, suboptimum therapy adherence, drug–drug interaction, access and affordability of health services and side effects like vomiting.18
In our study, distribution of average HbA1c values (<7.0, 7.0–8.0 and >8.0) were 12.2%, 6.6% and 51.7%, respectively. We observed that HbA1c<7 group was having minimal risk for TB. The diabetics with HbA1c>7 were at twice, higher risk for TB. Comparing with Leegaard et al. study, average HbA1c in the similar groups (<7.0, 7.0–8.0 and >8.0) were 1.8%, 0.7% and 1.6% respectively, which was found to be much lower compared to our study. However, 94% of the subjects were non-diabetics in their study.19 Similar results as our study was reported by Leung et al., which states that patients with HbA1c value >7 are at two fold higher the risk of active TB.20
Several mechanisms have been proposed to explain the high risk of TB in DM. Diabetics are vulnerable to TB due to impaired monocyte chemotaxis, reduced interferon (IFN γ) and activation of alveolar macrophages, diminished type 1 cytokine expression, and innate immunity.20
The growth and infection of M. tb in cells depend on the innate and adaptive immune responses of the host. The host cell phagolyses bacteria by the generation of reactive nitrogen and oxygen species. This autophagy pathway is regulated by mTOR complex-1, serine/threonine kinase, and AMPK. Singhal et al. reported that metformin-induced activation of AMPK inhibits mycobacterial growth in macrophages. Hence, it was suspected to have potential effect on anti-tubercular regimen in diabetics due to its role in maintaining the phagosomal pathway and promoting antibacterial action.11
Our study has demonstrated that the patients who were on metformin had a protective effect against tuberculosis 3.9 times compared to other hypoglycemic treatment regimens. But, we found both 500mg (25.7%) and 1000mg (27.3%) of metformin doses have no difference in protective action. Hence, the study exhibits metformin can exert protective action against TB, irrespective of different doses of the metformin. It was found that metformin was part of the prescription in just 25.3% of SG and 57.1% of the CG. Metformin should be included in the therapy for all type 2 DM patients, if tolerated and not contraindicated, as it is the only oral anti-hyperglycemic medication proven to reduce the risk of total mortality, according to the United Kingdom Prospective Diabetes Study (UKPDS).
ConclusionThe study concludes that metformin has protective effect in diabetic patients against tuberculosis infection. Acid-fast bacilli were dominantly found to be positive among higher HbA1c (>8%). Poor glycemic control was associated with increased risk of TB infections. This protective effect of metformin against tuberculosis is not dose dependent. Due to poor medication history documentation, we were not able to gather duration of metformin use. Hence, we were not able to assess metformin usage duration relationship with its protective action. However, we found a positive correlation with single and/or short-term exposure of metformin can produce long term immunity against TB infection.
Ethical approvalInstitutional Ethical Clearance obtained from Kasturba Hospital (KH), Manipal, India (IEC 430/2015).
Conflicts of interestThe authors declare no conflicts of interest.
We express our gratitude to Manipal College of Pharmaceutical Sciences and Kasturba Medical College, Manipal University, Manipal for the support.
