

This study aimed to estimate the prevalence of infection by the hepatitis B virus (HBV) and hepatitis C virus (HCV) in people infected by the human immunodeficiency virus (HIV) and analyze sociodemographic and behavioral factors associated with such co-infection. A cross-section study was performed in 495 individuals treated at a public center in the city of Goiânia. Participants were interviewed and blood collected for evaluation of serological and molecular markers for HBV and HCV. The rate of exposure to HBV was 33.5% (95% CI 29.4–37.9). Nineteen patients (3.8%) were diagnosed as HBV carriers, of whom 68.4% were HBV DNA positive. The prevalence of anti-HCV was 9.7% (95% CI 7.3–12.7). Genotype 1a was identified in 72.7% of the PCR samples positive for HCV. Co-infection by all three viruses was 4.4% (95% CI 2.9–6.8). Being, male, aged ≥40 years, history of sexually transmitted disease (STD), and having homosexual practices were independently associated with the presence of markers of HBV exposure. A history of injectable drugs use and STDs showed association with HCV seropositivity. Approximately 50% of participants were not aware of their HBV and HCV serostatus. The results obtained may contribute to assess the burden of viral hepatitis in people living with HIV and to guiding preventive measures for more vulnerable groups.
Hepatitis B (HBV) and C (HCV) viruses are responsible for the most common chronic viral infections worldwide. The prevalence of HBV and HCV infection is higher among people living with the human immunodeficiency virus (HIV) compared to the general population due to the common transmission routes and the overlap of behavioral risk factors for these viruses.1 Guidelines for the clinical management of HIV patients recommend testing for infection markers for viral hepatitis, and clinical evidence shows that co-infections are associated with worse prognosis of the liver disease.2,3
The investigation of the presence of HBV and HCV in HIV infected patients is important from the public health perspective to measure the resources required for prevention and treatment. Currently, HIV infected patients have greater longevity due to effective antiretroviral regimens as well as more effective drugs to treat hepatitis B and C. Thus, estimating the magnitude of co-infection in different populations is relevant.
The prevalence of HIV-HBV or HIV-HCV co-infection presents great variation and reflects differences in the sociodemographic profile, lifestyle, and hepatitis B immunization coverage in different population groups. A recent systematic review of the national literature showed that the prevalence of HCV infection among HIV infected individuals ranges from 3.3 to 82.4%.4 It is worth noting that most estimates of prevalence of HIV and hepatitis B and C co-infections were obtained in the South and Southeast regions of Brazil. This study aimed to estimate the prevalence of HBV and HCV infection among HIV-infected individuals and to investigate factors associated with co-infection in the state of Goiás. These results may contribute to assessing the burden of viral hepatitis in people living with HIV and to guiding preventive measures for more vulnerable groups.
MethodsThis cross-sectional study included HIV-infected patients, aged 18 years or more, treated at public health services in the city of Goiânia, state of Goiás, Brazil. The participants were recruited sequentially from March to May 2011 until achieving the necessary sample size. A sample of 450 patients was considered to be sufficient to detect prevalence of 2,0% for HBV (anti-HBc) and HCV (anti-HCV) infection, with 1% precision and a 95% confidence interval (95% CI).
After signing the informed consent form, participants underwent a structured interview to investigate sociodemographic, clinic and behavioral variables potentially associated with co-infection. Blood was collected to perform laboratory tests. Enzyme immunoassays were performed (3rd generation ELISA) to search for serological markers of hepatitis B (total anti-HBc, HBsAg, anti-HBs) and hepatitis C (anti-HCV). HBV DNA was assayed (PCR – Real Time) in all HBsAg-positive samples. HCV viral load was quantified (PCR – Real Time) in all anti-HCV-positive samples. We considered the presence of HCV RNA as a marker of infection activity. HCV genotyping and subtyping (PCR – Real Time) were performed for all samples that showed detectable HCV RNA. The history of antiretroviral drug use was obtained from the records of distribution centers of these drugs. CD4 T lymphocytes and HIV-1 viral load quantification values were obtained from the records of the Central Laboratory (Laboratório Central – LACEN) – Goiás.
The prevalence of HBV and/or HCV infection, with their respective 95% CI, were estimated. A univariate analysis was performed to evaluate the relationship between outcome variables (positive for HBV or HCV) and different exposure variables (sociodemographic and behavioral variables). The Odds Ratios (ORs) and their respective 95% CI were calculated. The variables that reached a significance level lower than 0.10 for association with HBV or HCV positivity in the univariate analysis were included in the logistic regression model, and the adjusted OR was calculated. In the multivariate analysis, a significance level lower than 0.05 was established. The statistical software SPSS 15.0 was used. The project was approved by the Ethics and Research Committee of the Pontifical Catholic University of Goiás.
ResultsThis study included 495 individuals, of which 366 were male (73.9%). The age of the participants ranged from 18 to 70 years (median age of 40 and interquartile range from 32 to 47 years). Previous use of injectable drugs was reported by 4.6% of men and 0.8% of women (p<0.05). Sexual intercourse with drug users was reported by 5.2% of men and 14.5% of women (p<0.01). History of blood transfusion and tattoos was reported by 13.9% and 18.8% of individuals, respectively, with no differences between men and women. Approximately half of the participants (n=221) reported at least one episode of sexually transmitted disease, most frequently gonorrhea (n=95) and syphilis (n=83). The median period since HIV diagnosis was six years with an interquartile range from two to 10 years. The use of antiretroviral therapy was reported by 74.9% of participants.
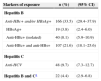
The prevalences of hepatitis B and C are presented in Table 1. The presence of at least one marker of exposure to the hepatitis B virus (anti-HBc and/or HBsAg) was detected in 166 participants, resulting in a prevalence of 33.5% (95% CI 29.4–37.9). Nineteen patients (3.8%; 95% CI 2.4–6.0) were HBsAg-positive, of whom 13 (68.4%) were positive for HBV DNA detection. Among the 19 HBsAg-positive individuals, 10 (52.6%) were not aware of their HBV infection. The prevalence of HCV infection was 9.7% (95% CI 7.3–12.7), and 54.2% of HCV ELISA positive individuals were not aware of their serostatus. For quantitative HCV RNA, of the 48 anti-HCV-positive individuals, 22 (45.8%) had a detectable viral load, ranging from 598 to 6,288,232copies/mL. The frequency of HCV genotypes was 86.4% for genotype 1 (72.7% of subtype 1a and 9.1% of subtype 1b) and 13.6% for genotype 3. Of the 22 individuals with detectable viral load for HCV, four did not know they were infected, and of the 18 who knew, 11 reported being treated for hepatitis C. Twenty-two participants showed markers of exposure to hepatitis B and C viruses, which resulted in a prevalence of co-infection of 4.4% (95% CI 2.9–6.8).
Prevalence of serological markers of exposure to hepatitis B and C viruses in 495 HIV-infected individuals treated in a public health center of Goiânia – Goiás.
| Markers of exposure | n (%) | (95% CI) |
|---|---|---|
| Hepatitis B | ||
| Anti-HBc+ and/or HBsAg+ | 166 (33.5) | (29.4–37.9) |
| HBsAg+ | 19 (3.8) | (2.4–6.0) |
| Anti-HBc+ (isolated) | 40 (8.1) | (5.9–10.9) |
| Anti-HBc+ and anti-HBs+ | 107 (21.6) | (18.1–25.6) |
| Hepatitis C | ||
| Anti-HCV | 48 (9.7) | (7.3–12.7) |
| Hepatitis B and Ca | 22 (4.4) | (2.9–6.8) |
n, number of cases; 95% CI, 95% confidence interval; +, positive.
Table 2 presents the results of the univariate analysis for factors potentially associated with markers of exposure to HBV (HBsAg and/or total reactive anti-HBc) or HCV (anti-HCV). After multivariate analysis, male individuals (adjusted OR=2.0; 95% CI 1.1–3.8), age equal to or higher than 40 years (adjusted OR=2.4; 95% CI 1.5–3.8), reported history of sexually transmitted diseases (STDs) (adjusted OR=1.9; 95% CI 1.2–2.9), and homosexuality or bisexuality (adjusted OR=3.7; 95% CI 2.2–6.3) were independently associated with a significantly higher risk of having markers of HBV infection. Patients with a history of STDs had almost three times higher risk of being anti-HCV positive (OR=2.7; 95% CI 1.4–5.4) compared with patients who denied having STDs. A history of injectable drugs use was associated with almost 12-fold the risk of HCV infection (anti-HCV positive) compared with individuals who did not use drugs (OR=11.8; 95% CI 3.9–35.8).
Univariate analysis of factors associated with exposure to hepatitis B (HBV) and C (HCV) viruses in 495 HIV-infected individuals treated in a public health center in Goiânia – Goiás.
| Risk factors | Exposure to HBVa | OR (95% CI) | p | Exposure to HCVb | OR (95% CI) | p | ||
|---|---|---|---|---|---|---|---|---|
| Yes | No | Yes | No | |||||
| Gender | ||||||||
| Male | 149 | 217 | 4.5 (2.6–7.8) | <0.01* | 35 | 331 | 0.9 (0.5–1.8) | 0.87 |
| Female | 17 | 112 | 13 | 116 | ||||
| Age | ||||||||
| ≥40 years | 102 | 157 | 1.7 (1.2–2.6) | <0.01* | 26 | 233 | 1.1 (0.6–2.0) | 0.79 |
| <40 years | 64 | 172 | 22 | 214 | ||||
| Education | ||||||||
| <9 years | 53 | 130 | 0.7 (0.5–1.1) | 0.10* | 22 | 161 | 1.5 (0.8–2.7) | 0.18 |
| ≥9 years | 113 | 199 | 26 | 286 | ||||
| Presence of tatoo | ||||||||
| Yes | 28 | 65 | 0.8 (0.5–1.3) | 0.44 | 12 | 81 | 1.5 (0.8–3.0) | 0.25 |
| No | 138 | 264 | 36 | 366 | ||||
| History of blood transfusionc | ||||||||
| Yes | 24 | 45 | 1.1 (0.6–1.8) | 0.84 | 9 | 60 | 1.5 (0.7–3.2) | 0.32 |
| No | 142 | 281 | 39 | 384 | ||||
| History of STDd | ||||||||
| Yes | 100 | 121 | 2.6 (1.8–3.8) | <0.01* | 34 | 187 | 3.4 (1.8–6.4) | <0.01* |
| No | 66 | 207 | 14 | 259 | ||||
| IDU | ||||||||
| Yes | 6 | 12 | 1.0 (0.4–2.7) | 0.99 | 10 | 8 | 14.4 (5.4–38.7) | <0.01* |
| No | 160 | 317 | 38 | 439 | ||||
| Sex with IDUe | ||||||||
| Yes | 8 | 29 | 0.5 (0.2–1.1) | 0.09* | 7 | 30 | 2.3 (1.0–5.6) | 0.06* |
| No | 158 | 291 | 41 | 408 | ||||
| Sexual orientation | ||||||||
| Homo/bisexual | 95 | 91 | 3.5 (2.4–5.2) | <0.01* | 14 | 172 | 0.7 (0.3–1.3) | 0.21 |
| Heterosexual | 71 | 238 | 34 | 275 | ||||
| Time of HIV diagnosisf | ||||||||
| ≥6 years | 86 | 163 | 1.1 (0.7–1.6) | 0.66 | 29 | 220 | 1.6 (0.9–2.9) | 0.14 |
| <6 years | 80 | 165 | 19 | 226 | ||||
| Exposure to HCVb | ||||||||
| Yes | 22 | 26 | 1.8 (1.0–3.2) | 0.06* | – | – | – | – |
| No | 144 | 303 | – | – | ||||
OR, odds ratio; 95% CI, 95% confidence interval; p, significance (<0.10).
The prevalence of co-infection with the hepatitis B and C viruses was estimated in a population of adults with a predominance of males whose exposure route to HIV was mostly sexual. The prevalence of HBV carriers (HBsAg) was 3.8% and of anti-HCV was 9.7%. These prevalences are six to seven fold higher than the rates found in a population-based study conducted in capital cities of the Midwest.5,6 These results indicate a high potential morbidity burden in the coming years due to co-infection with HIV and viral hepatitis.
In Brazil, studies conducted with HIV-infected individuals have found prevalences of HBsAg or anti-HBc carriers ranging, respectively, from 3.7 to 27.3% or from 38.6 to 55.1%.7–10 These differences probably reflect the percentage of risk factors in the studied groups and the endemicity pattern for HBV in different regions. In this study, 3.8% (95% CI 2.4–6.0) of participants were carriers of the hepatitis B virus, and HBV DNA was detected in approximately 65% of HBsAg-positive cases. Since hidden HBV infection was not investigated in this study, this may have underestimated the prevalence of HBV-infected individuals.11 Moreover, a negative result of the molecular test does not rule out the presence of the virus because viremia may be undetectable or temporarily suppressed due to antiretroviral drugs. The Brazilian Immunization Program recommends that HIV-infected individuals should be investigated for HBV infection and the susceptible ones should be vaccinated. The present study was not designed to assess vaccine coverage or lost opportunities for immunization against HBV, thereby, anti-HBs was investigated only in anti-HBc positive patients.
Regarding the factors associated with HBV infection in people living with HIV, the results of this study are consistent with the national and international literature, in which higher prevalence of HBV were described in older male individuals with homosexual practices. The association between older age groups and HBV is a well-known and widely observed fact resulting from the increased risk of exposure with time and the greater vaccination coverage in younger populations.1,12
Less than 5% of participants reported a history of injectable drugs use, and the prevalence of HCV was 9.7%. Conversely, in studies conducted in the South and Southeast regions of Brazil, from 20 to 100% of participants were injectable drug users (IDUs), and the percentage of individuals co-infected with HCV reached 80%.9,13 Although the percentage of IDUs in this sample is small when compared with these studies, the use of injectable drugs still exhibited a strong association with HCV-positivity, which is consistent with the literature. Also, the association between HCV and the history of STDs was supported by the study, which indicates the importance of the sexual transmission of HCV through unprotected sex.14,15
HCV RNA was detected in approximately half of anti-HCV-positive samples. We assume that the absence of HCV RNA is indicative of previous infection with elimination of the virus (permanent or temporary) or represents a false-positive result of the serological test used for triage, although all anti-HCV-positive samples had been tested in duplicates. Similar results were described with percentages close to 50% detection of HCV RNA in anti-HCV-positive samples in other studies in Brazil.16,17 In contrast, HCV RNA was detected in approximately 90% of HIV-positive individuals who had never been treated for HCV13 in the South region. The variations in the proportion of HCV RNA detection in anti-HCV samples in different studies probably reflect methodological differences, which include the degree of exposure to antiretroviral drugs in different population groups.
Regarding the genotypic profile of HCV, we identified a predominance of genotype 1, followed by genotype 3. The predominance of genotype 1 is consistent with results obtained in various studies conducted in Brazil.13,16,18,19 Genotype 1 has a worse therapeutic response than genotypes 2 and 3.2,3 Genotype 3 and subtype 1a have been associated with transmission in IDUs.16,17,20 The presence of genotype 3 in the population studied could indicate the importance of injectable drugs for HCV transmission in HIV-infected patients. However, the study was not designed to analyze the association between genotypes and the HCV transmission route.
It is noteworthy that 50% of patients with positive serology for HBsAg or anti-HCV reported not knowing they were infected. These results do not allow us to state that these patients had not been previously examined or counseled regarding these infections because they were all being followed-up in specialized reference centers. This population might require a differentiated approach to minimize loss of opportunities for treatment and transmission reduction.
Some limitations of this study are inherent to cross-sectional studies, making it difficult to establish a temporal relationship between co-infections and potential exposure variables. Although the sample was not random, individuals were recruited in the main specialized diagnosis public center, where almost all HIV-infected patients of the municipality undergo periodic tests to monitor the HIV viral load and CD4 count.
Despite the methodological limitations mentioned, this study allowed for prevalence estimation and delineation of the profile of HIV-infected patients co-infected with the hepatitis B and C viruses treated in public centers of Goiás. The results obtained indicate the need for future studies that allow reducing the clinical and economic impact of long-term co-infections in this population.
Conflicts of interestThe authors declare no conflicts of interest.
