

To investigate the prevalence of human polyomavirus (BK and JC viruses) infection in peripheral blood mononuclear cells of healthy blood donors.
MethodsThe study included 250 healthy blood donors. Five-milliliter blood was drawn into sterile EDTA tubes and PBMCs were isolated from whole blood. The isolated PBMCs were counted and stored at −70°C for future investigation. DNA was extracted and subjected to simple, sensitive and specific semi-nested PCR as well as QPCR using both general and specific primers for different assays.
ResultsOf 250 blood samples, 66 (26.4%) were positive for BKV DNA (146–34,514 copies/106 cells). JC DNA was found in 45 (18%) blood samples (65–21,250 copies/106 cells). Co-infection with these viruses were found in 11 (4.4%) out of 250 blood samples.
DiscussionOur study provides important data on polyomavirus infection in peripheral blood mononuclear leukocytes in immunocompetent individuals. These data indicate significant differences between the prevalence of BKV and JCV infection in healthy blood donors. The prevalence of BK and JC virus infection is higher in the age range 30–39 years compared to other age ranges.
The human polyomavirus BKV and JCV are prevalent globally in populated areas but are not easily transmitted. Seroconversion to BKV infection occurs early in life (5–7 years) while to JCV occurs later. Human polyomavirus viruses, small, non-enveloped DNA, infect immunocompetent individuals without specific signs or symptoms. They are able to establish subclinical and persistent infections and may reactivate from latency in case of immunosuppression.1–4 Viral infection is persistent and usually established in the kidney with high levels of virus being excreted in the urine.
JCV reactivation in immunocompromised patients may cause a demyelinating disease of the central nervous system (CNS), named progressive multifocal leukoencephalopathy (PML), whereas BKV reactivation may cause hemorrhagic cystitis and polyomavirus associated nephropathy (PVAN) in renal transplant patients.5,6 Since no specific antiviral drugs are available to treat polyomavirus disease, treatment depends on improving immune functions to regain control over viral replication.7
The main sanctuary of BKV and JCV persistence in healthy subjects is the kidney. However, identification of BKV and JCV DNA in peripheral blood mononuclear cells (PBMC) likely indicates recent infection by or re-activation of these viruses.8,9 The first evidence of an interaction between BKV and hematopoietic cells was given by studies on the stimulatory effect of BKV infection on lymphocyte cultures and on BKV receptors on the surface of peripheral blood cells. These data suggested the participation of lymphoid cells in the pathogenesis of BKV infection. Nevertheless, the data on the prevalence of BKV and JCV DNA in peripheral lymphocytes is highly discordant and contradictory. Blood BKV positivity varies from 0 to 90%.10,11 Moreover, detection of BKV sequences in lymphocytes has disputable significance for the pathogenesis, as it is not yet clear whether these cells are persistently or transiently infected and had integrated or episomal copies of viral DNA. It is reported that 2–3% of the population have JCV in their PBMC, particularly in B-lymphocytes. However, the likelihood of secondary transmission is unknown. Overall, immunocompromised patients, pregnant women, diabetics, and the elderly appear to be at higher risk of disease and transmission of polyomaviruses.
Polyomavirus infection and viral replication have been reported in plasma and urine samples of healthy, immunocompetent blood donors. However, transmission by blood transfusion has not been documented.12 Since a number of immunocompromised transplant recipients need blood transfusion during organ transplantation procedure, the transfused blood maybe contaminated with an active form of the virus. We investigated the prevalence of polyomavirus BKV and JCV infection in healthy blood donors. Moreover, the DNA level at the time of blood donation was determined by real-time polymerase chain reaction.
MethodsStudy population and the samplesA total of 250 healthy blood donors randomly selected at the blood donation center, Shiraz, Iran, were included from September through December 2017, and categorized into four age groups (20–29, n=44, 30–39, n=85, 40–49, n=67, and 50–59 years, n=54). There were only 11 females (age 19–57 years). Included donors were negative serologies for hepatitis B virus (HBV), hepatitis C virus (HCV), HIV, and Treponema pallidum infections. Participants gave written informed consent and the study was approved by the local ethics committee.
From each participant, 5mL of blood was collected into sterile EDTA tubes at the time of regular blood donation. Peripheral blood mononuclear cells (PBMCs) were isolated using Ficoll-Paque™ (GE Healthcare, Uppsala, Sweden) gradient centrifugation (density 1.077g/mL) and stored at −70°C for future investigation.
Semi-nested PCRDNA extraction and PCR amplificationpBKV (34-2) plasmid (ATCC® 45025) and pJCV (1–4) plasmid (ATCC® 45027™) was used as the reference source of DNA for the PCR assays. Viral DNA from PBMCs was extracted using commercially available QIAmp DNA Blood Mini kit (Qiagen, Hilden, Germany). For the amplification of target genes, PCR was run in two separate steps, as described previously.14 The outer primers were used to amplify parts of the conserved early regions for both virus genomes. PCR amplification was carried out with 0.5–0.8μg of extracted DNA from 1×106 PBMCs, 1× PCR buffer, 1.5mM MgCl2, 200μM of dNTPs, 0.5μM of each outer primer (PEP1 and PEP2), and 2.5U of Taq DNA polymerase, in a final volume of 50μL. The outer primer pair 5′-AAGTCT TTA GGG TCT TCT AC-3′ and 5′-GTG CCA ACCTAT GGA ACA GA-3′ was used to amplify a 176-bp fragment common to both viruses. For specific detection, the inner primer pair combined the common primer 5′-AAG TCT TTA GGG TCT TCT AC-3′ with either the BKV-specific primer 5′-GAG TCC TGG TGG AGT TCC-3′ to obtain a BKV fragment of 149bp, or the JCV specific primer 5′-GAA TCC TGG TGG AAT ACA-3′ yielding a JCV fragment of 146bp. Thermal cycler conditions were as follows: a first denaturing cycle at 94°C for 5min, followed by 40 cycles of amplification defined by denaturation at 94°C for 30s, 55°C annealing temperature for 45s, and extension at 72°C for 1min. A final extension cycle of 72°C for 5min was included.
In a second-round PCR, 1μL of the 1:10-diluted first round PCR product was amplified under the above same condition with the specific inner primer pairs. The reaction was visualized on 2% agarose gel and stained with GelRed™ and visualized under UV light.
To investigate efficient DNA extraction and PCR amplification, human β-actin gene was also amplified along with the samples using primers, which amplified a 177-bp fragment. Only positive samples were investigated further for amplification of the target DNA sequences.
SYBR green-based real-time PCR assayA SYBR green-based real-time qPCR assay, targeting the highly conserved regions of BKV and JCV genomes, was developed for detection and quantification of BKV and JCV DNA extracted from PBMCs. Using SYBR green PCR master mix from Takara (Shiga, Japan), the optimization of the PCR reaction was performed by determining the optimal amount of primers, as well as the cycling condition. Quantitative real-time PCR was performed in a final volume of 25μL using Qiagen Rotor-Gene Q 5-Plex (QIAGEN, Hilden, Germany). The outer forward primer 5′-AAGTCT TTA GGG TCT TCT AC-3′ of semi-nested PCR (0.2μM/reaction) with either the BKV-specific primer 5′-GAG TCC TGG TGG AGT TCC-3′ or the JCV specific primer 5′-GAA TCC TGG TGG AAT ACA-3′ (0.2μM/reaction) was used for amplification in real-time PCR assay. The DNA from clinical samples was extracted as described above (Section 2.2.1) and tested (2μL/reaction) in duplicate with the QPCR assay.
Thermal cycling was initiated with incubation at 95°C for 10min, followed by 40 cycles of 95°C for 30s, 55°C for 30s, and 72°C for 30s, at the end of which fluorescence was read. A non-template control was included to monitor possible contamination.
Calibration curveFor the calibration curve, the threshold cycle (Ct) values were plotted against the logarithm of ten-fold serial dilutions of a plasmid containing the BKV (6×106 to 6×100 copies/reaction) and pJCV (1–4) plasmid (9×16 to 9×100 copies/reaction).
Data analysisThe statistical package SPSS Version 17.0 for Windows (SPSS, Chicago, IL, USA) was used data analysis. The associations with the studied categorical variables and BKV and JCV infection were assessed using X2 test or Fisher's exact test, when indicated.
ResultsLimit of detectionThe limit detection of the semi-nested PCR assay for BKV and JCV DNA was six and nine copies of plasma DNA/reaction, respectively. Serial 10-fold dilutions of pBKV and pJCV were run in QPCR. Standard curves displayed a linear relationship for qPCR assay, with efficiencies of 99% for both BKV and JCV targets. Under these conditions, the limits of detection were 1–60 copies/PCR reaction for both BKV and JCV DNA. No cross-reactions were found when BKV primers were used against JCV DNA and vice versa.
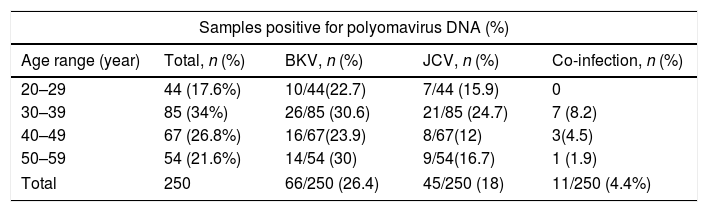
Prevalence of BKV and JCV DNA in PBMCsSemi-nested PCR was carried out carefully to avoid possible cross-contamination of BKV and JCV DNA. All the samples showed a positive result in the β-actin PCR, indicating absence of inhibitors and adequate amount of DNA. None of the negative controls was amplified. Results from semi-nested PCR for detection of BKV and JCV DNA in all samples are presented in Table 1. Overall, polyomaviruses BK and JC DNA were found in 111/250 PBMCs (44.4%) of healthy blood donors. BKV and JCV DNA were found in 66/250 (26.4%) and in 45/250 samples (18%), respectively. Distribution of BKV and JCV infection in various age ranges is shown in Table 1.
Prevalence of BKV and JCV DNA in peripheral blood leukocytes of healthy blood donors.
| Samples positive for polyomavirus DNA (%) | ||||
|---|---|---|---|---|
| Age range (year) | Total, n (%) | BKV, n (%) | JCV, n (%) | Co-infection, n (%) |
| 20–29 | 44 (17.6%) | 10/44(22.7) | 7/44 (15.9) | 0 |
| 30–39 | 85 (34%) | 26/85 (30.6) | 21/85 (24.7) | 7 (8.2) |
| 40–49 | 67 (26.8%) | 16/67(23.9) | 8/67(12) | 3(4.5) |
| 50–59 | 54 (21.6%) | 14/54 (30) | 9/54(16.7) | 1 (1.9) |
| Total | 250 | 66/250 (26.4) | 45/250 (18) | 11/250 (4.4%) |
The overall prevalence of BKV DNA was significantly higher than that of JCV DNA in PBMCs of healthy blood donors (p=0.03). Although the frequency of both BKV and JCV infections were higher in age range 30–39, no statistically significant differences were found related to age group (p>0.05). Among the 11 female healthy blood donors, BKV and JCV DNA were found in PBMCs in six (54.5%) and two (18%), respectively; with co-infection in two of them. BK and JC virus DNA were not detected in blood samples of three female blood donors. On the other hand, the incidence of BKV and JCV infection in male donors were 59/239 (24.9%) and 42/239 (17.6%), respectively.
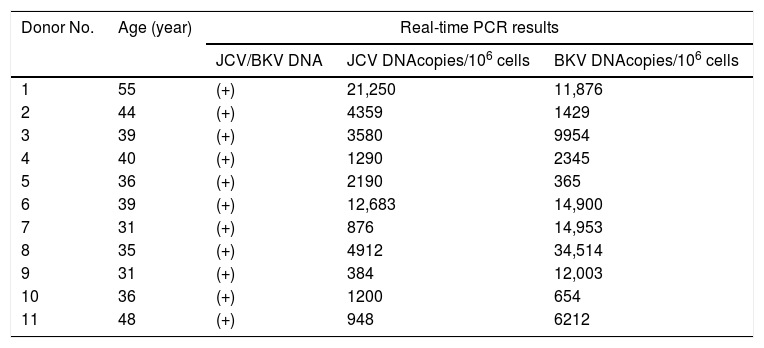
BK and JC DNA viral load in semi-nested PCR positive PBMCs samplesIn order to measure viral load, all semi-nested positive samples were tested by quantitative real-time PCR. Among the 66 PBMC samples positive for BKV DNA with semi-nested PCR, viral load ranged from 146×100 to 34×103 copies/106 PBMC by SYBR green real-time PCR. For JCV, viral load ranged from 65×100 to 21×103 copies/106 PBMCs. Mean viral load for BKV and JCV DNA/106 copies of PBMN were 5773.56 and 3652.92 with the mode of 654 and 952 respectively.
Results of QPCR for the samples with co-infection of BKV and JCV are shown in Table 2.
Viral load of BKV and JCV co-infected PBMCs samples.
| Donor No. | Age (year) | Real-time PCR results | ||
|---|---|---|---|---|
| JCV/BKV DNA | JCV DNAcopies/106 cells | BKV DNAcopies/106 cells | ||
| 1 | 55 | (+) | 21,250 | 11,876 |
| 2 | 44 | (+) | 4359 | 1429 |
| 3 | 39 | (+) | 3580 | 9954 |
| 4 | 40 | (+) | 1290 | 2345 |
| 5 | 36 | (+) | 2190 | 365 |
| 6 | 39 | (+) | 12,683 | 14,900 |
| 7 | 31 | (+) | 876 | 14,953 |
| 8 | 35 | (+) | 4912 | 34,514 |
| 9 | 31 | (+) | 384 | 12,003 |
| 10 | 36 | (+) | 1200 | 654 |
| 11 | 48 | (+) | 948 | 6212 |
Descriptive statistics of BK and JCV detection in total samples are shown in Table 3.
DiscussionThe present study shows a high frequency of BKV and JCV DNA in PBMC of healthy blood donors. Peripheral leukocytes were isolated from blood samples of healthy individuals and cellular DNA was extracted. The prevalence of BKV and JCV DNA in peripheral leukocytes from 250 healthy adult blood donors was evaluated by semi-nested PCR. The sensitivity and specificity of the method using specific inner PCR primers allow us to determine if these viruses were present in the sample tested.
In addition to the kidney, several studies have demonstrated that peripheral blood leukocytes are common sites of latent BKV and JCV infection in healthy individuals. However, persistence of BKV and JCV polyomaviruses in lymphocytes of healthy humans is still debated. The rate of PBMC infection by BKV and JCV have been reported between 0 to 90% in the various studies.10,13–17 In our investigation, the overall detection of BKV and JCV DNA in PBMC of healthy blood donors was 24.6 and 18%, respectively, which is the first report from our geographical region. In one study in China, using semi-nested PCR assay with the same primers used in our study, BKV and JCV DNA was reported in 42.1% and 7.8% of PBMC from healthy blood donors, respectively (16). Such findings indicate that BKV and JCV infection in varies in different geographic areas of the world.
Furthermore, the results of this study point out that the prevalence of BKV DNA was highly significantly higher compared to that of JCV DNA (p=0.03). Because of the small sample of female blood donors (11/250 donors) the impact of sex on the results could not be ascertained, BK virus infection seemed to be more common than JC virus infection (3:1). Although the prevalence of BKV and JCV DNA in PBMC was higher in the age range 30–39 years, there was no statistically significant difference among age groups.
BK polyomavirus is associated with nephropathy and ureteric stenosis in kidney transplant recipients as well in other types of transplant recipients.18,19 BKV causes hemorrhagic cystitis in allogenic hematopoietic cell transplant recipients.20 However, less than 5% of polyomavirus nephropathy among kidney transplant recipients may be caused by JC, perhaps with more inflammation and focal fibrosis, and is typically associated with a milder clinical course.21
Generally, primary infection of BKV and JCV in healthy individuals is followed by lifelong viral persistence. Both of these viruses are shed in the urine of healthy people. However, immunosuppression may reactivate latent virus in healthy individuals and cause disease.
Real-time quantitative PCR was used to quantitate DNA of polyomaviruses BK (BKV) and JC (JCV) in PBMCs of healthy individuals. There is no standard level of polyomavirus DNA in healthy or even in patients. Many variables including sample processing protocol and sensitivity and specificity of detection methods may affect the ultimate results of quantitative PCR assays. Environmental factors such as age, sex, personal hygiene, individual's immune status can interfere with the result of the assay. Based on the findings of this study, the virus persists in blood mononuclear leukocytes in up to 25% of healthy blood donors who are lifelong carriers of the virus. It can be transmitted by transfusion of cellular blood components although this may be difficult to distinguish from reactivation of a previous infection. BKV infection, in particular, can cause severe infection in renal transplant and immunocompromised individuals. Therefore, polyomavirus disease transmitted through PBMCs during blood transfusion should not be neglected.
We have shown that BKV and JCV can infect PBMCs of healthy individuals and establish a latent infection. In our experiment, the DNA level in different individuals varies from 146×100 to 34×103 copies/106 PBMC for BKV and 65×100 to 21×103 copies/106 PBMC for JCV DNA. Therefore, when transfusing blood to an immunosuppressed patient transmission of the high level of infected cells with polyomavirus may result in severe disease.
In conclusion, our study provides important data on polyomavirus infection in peripheral blood mononuclear leukocytes in immunocompetent individuals living in the southwest of Iran. These data indicate significant differences between the prevalence of BKV and JCV infection in healthy blood donors. The prevalence of BK and JC virus infection is higher in the age range 30–39 years compared to other age ranges. Different levels of BK and JC virus DNA was found in PBMCs of healthy blood donors. However, viral DNA quantitation in plasma samples by real-time PCR helps identifying ongoing viral reactivation.
FundingThis research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of interestThe authors declare no conflicts of interest.
This research was supported by Shiraz University of Medical Sciences Grant Number 97-01-45-17407.
