
Neonatal septicemia is the most important cause of neonatal mortality. A wide variety of bacteria both aerobic and anaerobic can cause neonatal sepsis. Genus Pantoea is a member of Enterobacteriaceae family that inhabits plants, soil and water and rarely causes human infections, however, Pantoea dispersa has not been reported as a causative organism for neonatal sepsis. We hereby report two neonates with early onset sepsis caused by Pantoea dispersa. Early detection and appropriate antibiotic therapy can improve overall outcome of this rare infection in neonates.
Neonatal septicemia is the most important cause of morbidity and mortality among neonates worldwide. A wide variety of bacteria both aerobic and anaerobic can cause neonatal sepsis.1 Genus Pantoea is a member of Enterobacteriaceae family that inhabits plants, soil and water.2Pantoea agglomerans, member of this family, has previously been reported presenting as severe neonatal sepsis,3 however, Pantoea dispersa has not been reported as a causative organism for neonatal sepsis. We hereby report two neonates with early onset sepsis caused by Pantoea dispersa.
Case presentation 1A term, male baby presented at 48h of life with excessive cry, abnormal body movements and poor feeding. The baby was delivered by cesarean section due to breech presentation with 3060g birth weight and cried immediately after birth. Antenatal period was uneventful and mother had no risk factors for sepsis. Breastfeeding was started on day 1 of life and the baby accepted feeds well. At admission, the baby was sick looking, febrile and had hypoglycemic seizures (blood sugar 35mg/dL by dextrostix), which responded to dextrose bolus. Sepsis screen was positive with total leukocyte count 4500mm−3 and C-reactive protein 8mg/dL. The baby also had thrombocytopenia (platelet count 80,000mm−3) at admission. CSF examination, serum electrolytes and renal and liver function tests were normal (Table 1). The baby was started on first line antibiotics (piperacillin-tazobabctam with amikacin) along with glucose infusion rate at 8mg/kg/min. However, upper gastrointestinal bleeding started at 36h of life with worsening of thrombocytopenia (platelet count 24,000mm−3), following which antibiotics were upgraded to meropenem and amikacin and platelet concentrate was transfused, after which bleeding stopped. Coagulation profile was normal. Blood culture report showed Pantoea dispersae organism by automated Bact/Alert 3D system, which was sensitive to amikacin, cefepime, ceftriaxone, ciprofloxacin, meropenem and aztreonam, and resistant to cefazolin. Meropenem and amikacin were continued for 14 days. Platelet counts gradually improved and feeds were started on day 5 of life, with good tolerance. Ultrasonography of skull and abdomen were normal and the baby was discharged after 14 days of antibiotic therapy. At one month follow up, the baby was doing well and was gaining weight normally.
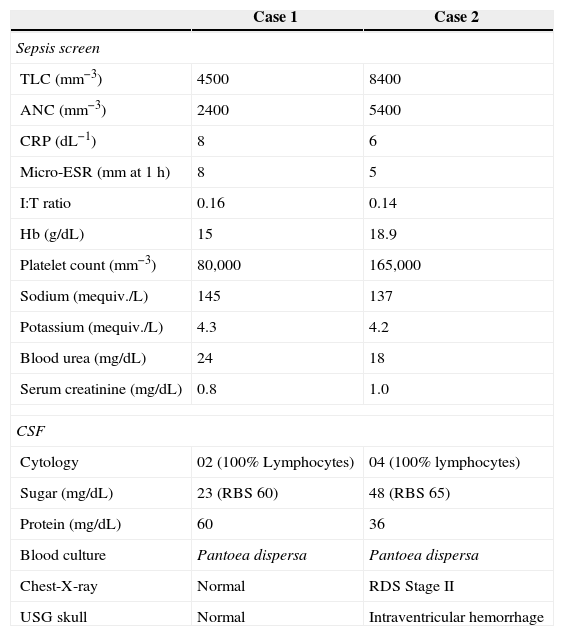
Initial investigations in both babies.
| Case 1 | Case 2 | |
|---|---|---|
| Sepsis screen | ||
| TLC (mm−3) | 4500 | 8400 |
| ANC (mm−3) | 2400 | 5400 |
| CRP (dL−1) | 8 | 6 |
| Micro-ESR (mm at 1h) | 8 | 5 |
| I:T ratio | 0.16 | 0.14 |
| Hb (g/dL) | 15 | 18.9 |
| Platelet count (mm−3) | 80,000 | 165,000 |
| Sodium (mequiv./L) | 145 | 137 |
| Potassium (mequiv./L) | 4.3 | 4.2 |
| Blood urea (mg/dL) | 24 | 18 |
| Serum creatinine (mg/dL) | 0.8 | 1.0 |
| CSF | ||
| Cytology | 02 (100% Lymphocytes) | 04 (100% lymphocytes) |
| Sugar (mg/dL) | 23 (RBS 60) | 48 (RBS 65) |
| Protein (mg/dL) | 60 | 36 |
| Blood culture | Pantoea dispersa | Pantoea dispersa |
| Chest-X-ray | Normal | RDS Stage II |
| USG skull | Normal | Intraventricular hemorrhage |
TLC, total leukocyte count; ANC, absolute neutrophil count; CRP, C-reactive protein; ESR, erythrocyte sedimentation rate; I:T ratio, immature to total cell ratio; CSF, cerebrospinal fluid; RBS, random blood sugar; RDS, respiratory distress syndrome.
Preterm (31 weeks), male baby was born by cesarean section for fetal distress with birth weight of 1210g. The baby cried immediately after birth and apgar scores were 7 and 8, at 1 and 5min, respectively. The mother had history of vaginal leaking for 24h prior to delivery, but there was no history of maternal fever, foul smelling liquor or pelvic tenderness. The baby had respiratory distress and grunting at birth with Silverman score 6/10, for which he was transferred to neonatal intensive care unit and put on nasal CPAP. Chest X-ray was suggestive of respiratory distress syndrome stage II, however, respiratory distress gradually improved on CPAP. Sepsis screen was negative at 6h. The baby was started on maintenance fluid and first line antibiotics (ampicillin–sulbabctam and amikacin) in view of positive risk factors for sepsis. However, the baby started deteriorating after 12h of life and had intracranial bleed and shock. His hematocrit decreased from 61% to 45% and platelet count decreased to 48,000mm−3. Packed red blood cell and platelet concentrates were transfused and vasopressors were started. Despite aggressive respiratory and vasopressor support, the baby expired at 24h of life. Blood culture report revealed growth of Pantoea dispersa organism by Bact/Alert 3D and Vi-Tech2 system, which was sensitive to amikacin, cefepime, ceftriaxone, ciprofloxacin, meropenem and aztreonam, and resistant to cefazolin.
A search for common source of the infection was initiated. The mother of second case had positive risk factors for sepsis; however, Pantoea dispersa is not a common human pathogen. Both babies were delivered in the same operation theater via cesarean section within a gap of 15 days; hence, cultures were sent from operation theater, which were all negative for Pantoea species. However, common source infection from operation theater was still suspected and operation theater was thoroughly fumigated after isolation of this organism. Over the last eight months following fumigation, no further case of Pantoea species sepsis has been reported from our microbiology laboratory.
DiscussionThe genus Pantoea belongs within the family Enterobacteriaceae and was proposed by Gavini et al. This complex covered many phena and genomic groups, some of which were later designated as new genera.2 Seven Pantoea species are currently distinguished: P. agglomerans, the prototype species of the genus; Pantoea ananatis; Pantoea stewartii (divided into the two subspecies Pantoea stewartii subsp. stewartii, and Pantoea stewartii subsp. indologenes); Pantoea dispersa; Pantoea citrea; Pantoea punctata; and Pantoea terrea. These species are generally associated with plants, either as epiphytes or as pathogens, and some species can cause disease in humans.4
Pantoea agglomerans (formerly Enterobacter agglomerans) is a gram-negative aerobic bacillus in the family Enterobacteriaceae. All species of the genus Pantoea can be isolated from feculent material, plants, and soil, where they can either be pathogens or commensals. Within the genus, P. agglomerans is the most commonly isolated species in humans, resulting in soft tissue or bone/joint infections following penetrating trauma by vegetation.5 As an opportunistic human pathogen, P. agglomerans can occur sporadically or in outbreaks. At the beginning of the 1970s, P. agglomerans (then called Enterobacter agglomerans) was implicated in a large U.S. and Canadian outbreak of septicemia caused by contaminated closures on bottles of infusion fluids; 25 hospitals were involved, with 378 cases. Since then, P. agglomerans bacteremia has also been described in association with the contamination of intravenous fluid, parenteral nutrition, the anesthetic agent propofol, blood products, and transference tubes used for intravenous hydration. Infection often occurs after injuries with plant thorns, wood slivers, or wooden splinters.4
Neonatal sepsis by Pantoea species is rarely reported. A recent report, which described the clinical picture of an almost fatal infection caused by P. agglomerans, was observed during an outbreak caused by contaminated parenteral nutritional fluids in a Malaysian neonatal intensive care unit in 2005. Seven of the eight infected neonates succumbed to the infection in this outbreak. P. agglomerans was isolated from cultures of the infected neonates and it spread by infected parenteral nutrition solutions.6 Two subsequent series afterwards reported eight neonates with late onset sepsis due to P. agglomerans, out of which five survived after appropriate antibiotic therapy.7,8
Pantoea dispersa has rarely been reported to cause human infection. In the first report, a 71-year old immunocompromised female patient with acute myeloid leukemia and multiple myeloma developed left focal lesion in lung fields with pleural effusion. Culture of bronchoalveolar lavage in this patient grew P. dispersa and the patient improved after adequate antibiotic therapy.9 In another report, two adult patients developed joint infection after total joint replacement, and the joint fluid culture revealed growth of P. dispersa. Contaminated sterilized saline used to process Gram stain was responsible for this pseudo-outbreak of P. dispersa.10
However, P. dispersa sepsis has not been reported in neonatal age group till now. Besides, this organism had not been reported from India till date. This is the first case report of P. dispersa presenting as neonatal sepsis from India to the best of our knowledge.
The organism was a Gram-negative, motile bacillus belonging to the family of Enterobacteriaceae. Species identification was done using automated Bact/Alert 3D system and antibiotic susceptibility was performed on Vi-Tech-2 system. Confirmation by molecular methods such as PCR could have been more specific, but they were not available in the facilities where the patients received care. In both cases, isolates showed in vitro susceptibility to commonly used antibiotics, had early onset sepsis, and showed significant clinical deterioration. The first baby was a term baby and improved well with antibiotic and supportive therapy. However, the second, was a preterm baby with other co-morbidities (respiratory distress syndrome and intracranial hemorrhage) and succumbed to disease despite early initiation of antibiotics.
To conclude, Pantoea species is a rare cause of neonatal sepsis. Early detection and appropriate antibiotic therapy can improve overall outcome.
Authors’ contributionVM and NG were involved in case management. VM and DY reviewed the literature and prepared the manuscript. JS and KS critically reviewed the manuscript. All authors have read and approved the final manuscript. VM will act as the guarantor of the report.
Conflicts of interestThe authors declare no conflicts of interest.
