





Meningococcal meningitis is a well established potential fatal infection characterized by fever, headache, petechial rash, and vomiting in the majority of cases. However, protean manifestations including abdominal pain, sore throat, diarrhea and cough, even though rare, should not be overlooked. Similarly, although disseminated infection could potentially involve various organ-targets, secondary immune related complications including joints or pericardium should be dealt with caution, since they remain unresponsive to appropriate antibiotic regimens. We hereby report the rare case of an otherwise healthy adult female, presenting with acute abdominal pain masking Neisseria meningitidis serotype B meningitis, later complicated with recurrent reactive pericarditis despite appropriate antibiotic treatment. There follows a review of current literature.
Meningococcal meningitis represents a severe – potentially fatal – infection characterized by fever, headache, petechial rash, and vomiting. Increased clinical suspicion and prompt diagnosis is pivotal to ensure favorable outcomes. However, uncommon manifestations including abdominal pain, cough, arthritis, vasculitis, or pericarditis can mislead the attending physician, while requiring combined treatment with agents other than appropriate antibiotics. Acute abdominal pain as initial manifestation of meningococcal infection is extremely uncommon, typically located around the right abdomen – commonly around the right iliac fossa. It can be commonly mistaken for acute cholecystitis, appendicitis, or mesenteric adenitis. Therefore, patients tend to initially present to surgical emergency departments. Pericarditis is also an uncommon (3–19%) but well-recognized complication of meningococcal disease.1 Presence of multiple factors differentiate between direct invasion by the organism (disseminated meningococcal disease with pericarditis or isolated meningococcal pericarditis), from an immune mediated reactive pericarditis (RMP).1 We hereby report the case of a 28-year-old otherwise healthy female presenting in our surgical department with acute abdomen masking meningococcal meningitis, later complicated by recurrent episodes of reactive pericarditis, despite appropriate antibiotic treatment.
Case reportA 28-year-old Caucasian female presented at our hospital complaining of fever, rigors, and severe epigastric pain, not subsiding following non steroid anti-inflammatory drug administration, during the last 24h. Upon admission the patient was in poor condition, BP:120/80mmHg, T: 38.8°C, GCS: 15/15, while physical examination revealed severe rebound tenderness along right upper quadrant and epigastrium. Blood tests came back to show WBC: 19.51K/μL (92.5/2.7/4.7%), PLT: 117.00K/μL, PT: 18.4s, INR: 1.59, and CRP: 26IU/L. Electrocardiogram (EKG) and chest-X-ray (CXR) were unremarkable. An emergency abdominal ultrasound and later CT scan did not reveal any cause of acute abdomen. Interestingly, the patient started complaining of headache during her stay in the emergency department. At the time, patient reassessment revealed increased nuchal rigidity and Kerning's sign suggestive of central nervous system involvement. Lumbar puncture revealed 15,200cells of polymorphonuclear predominance, Glu<5mg/dl and protein 530mg/dl in cerebrospinal fluid (CSF). CSF latex agglutination test and later CSF and blood cultures results showed Neisseria meningitidis group B sensitive to a range of antibiotics, hence the patient (following prior empiric therapy of vancomycin, ceftriaxone and dexamethasone) was put on ceftriaxone 4 gr qd. The patient presented dramatic clinical improvement a week following IV therapy with near normalization of inflammatory markers while serology for common viruses, including HIV and consecutive blood cultures came back negative. C3 and C4 complement concentrations were also normal. Ten days post-admission the patient started complaining of a sharp retrosternal pain radiating to the left scapula, associated with pericardial friction rub along the lower left sterna border. No alterations in hemodynamic, ABG, or other blood parameters including serum troponin I and creatine kinase MB were noted. However, EKG showed raised ST segments in leads V2–V6, indicative of pericarditis. Chest CT scan and cardiac ultrasound confirmed development of moderate pericardial effusion (Fig. 1A and B). In the context of previous clinical improvement, negative serology for infectious and autoimmune diseases, and presence of medication – sensitive meningococcus strain, we decided that pericarditis was immune- mediated and a combination of methylprednisolone and colchicine at 24mg and 0.5mg qd, respectively, was initiated. The patient showed clinical and radiologic improvement and was discharged 19 days post admission on a tapering scheme of corticosteroids (Fig. 1C). Interestingly, approximately one and a half months later – at the time on 4mg of methylprednisolone – the patient started complaining again of retrosternal pain. She visited a tertiary hospital where recurrence of moderate pericardial fluid was confirmed, while reinstitution of methylprednisolone 8mg/d and ibuprofen 600mg/tid was followed by gradual improvement and discharge shortly after. Since then, the patient has again presented in our department twice with recurrent pericarditis while on methylprednisolone tapering. After eight months of follow up and slow tapering scheme of corticosteroids and NSAIDs the patient remains in excellent condition, without symptoms and out of treatment.
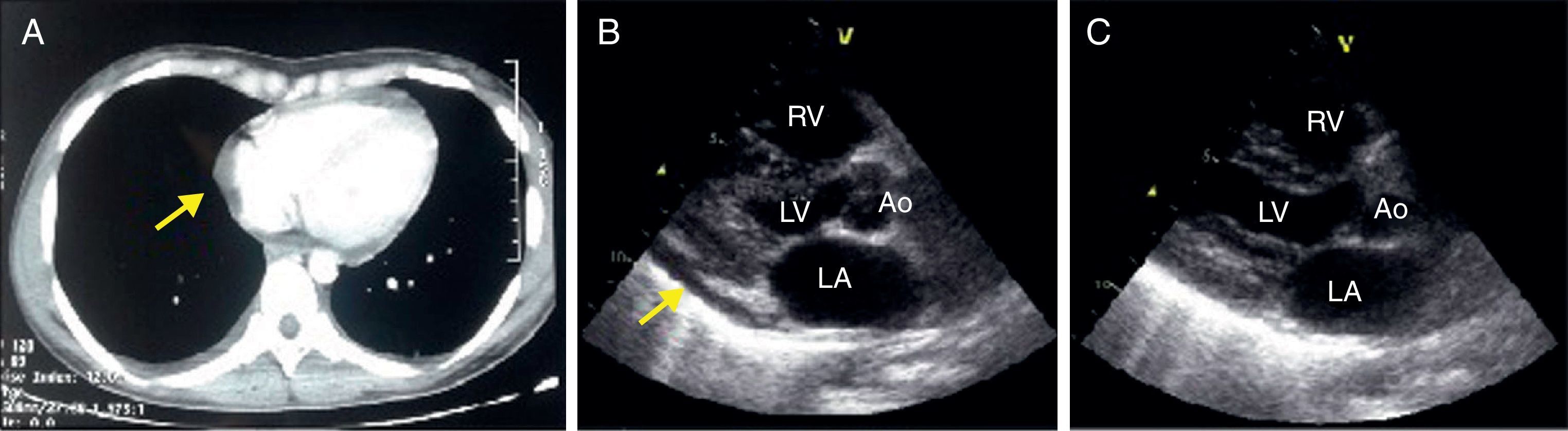
(A) Chest CT scan; (B) cardiac ultrasound (parasternal long axis view) revealed the presence of mild-to-moderate amount of pericardial effusion with no hemodynamic derangement (yellow arrows); and (C) no pericardial effusion was noted, following 9 days of corticosteroid therapy. Ao, aorta; LV, left ventricle; RV, right ventricle; LA, left atrium.
Acute abdominal pain as an initial manifestation of meningococcal infection is extremely uncommon, and can present both as an isolated entity, as well as in the context of meningococcal sepsis. Including ours, we have tracked no more than 19 cases of sharp abdominal pain as initial presentation of invasive meningococcal disease in global literature (Table 1). Despite equally involving adults and children, more than half (60%) of childhood cases are under six years of age.2–7 Based on available data, Neisseria meningitidis serotype C was the most frequently isolated pathogen (∼48% of cases).3,4,7–13 Two cases of serotype B, similar to our case, have also been identified, even though the former involving children.5,6 Fever was the most frequent accompanying symptom while a surgical procedure following suspicion of acute abdomen was conducted in 42% of these patients.3–5,7,8,11,14 The etiology of abdominal pain remains obscure. Several theories attempt to explain the underlying pathophysiology associated with this clinical entity including, mesenteric hypoperfusion, septic epiploic micro infarctions, splanchnic invasion via hematogenous spread or ascending infection from the urogenital tract, or immune complex deposition.2
Cases of meningococcemia presenting as acute abdomen since 1974.
| Reference | Year | Age (years) | Clinical manifestation | Serogroup | Site of isolation | Surgery |
|---|---|---|---|---|---|---|
| Our case | 2016 | 28 | Febrile | B | CSF, blood culture | No |
| Austin21 | 2015 | 33 | Febrile, vomiting & diarrhea | No data | Blood culture | No |
| san Alvarez2 | 2011 | 10 month | Febrile | A | Blood culture | No |
| Hsia9 | 2009 | 13 | Febrile, agitation | C | Blood culture | No |
| Tomezzoli5 | 2008 | 4 | Febrile | B | Blood culture | Yes |
| de Souza22 | 2006 | 6 | Febrile, myalgia | C | Peritoneal fluid | Yes |
| Herault8 | 2006 | 14 | Meningeal syndrome | C | Peritoneal fluid, blood culture | Yes |
| Kelly11 | 2004 | 28 | No data | C | Peritoneal fluid | Yes |
| Demeter23 | 1999 | 37 | Febrile | No data | Blood culture | No |
| 1999 | 34 | Febrile | No data | Blood culture | No | |
| Winrow6 | 1999 | 3 | Febrile | B | Blood culture | No |
| 1999 | 12 | Febrile | No data | Blood culture | No | |
| Schmid12 | 1998 | 21 | Meningeal syndrome, exanthema | C | Blood culture | No |
| Grewal10 | 1993 | 16 | Meningeal syndrome, exanthema | C | Blood culture | No |
| Kunkel4 | 1984 | 4 | Febrile | C | Peritoneal fluid | Yes |
| Bar Meir14 | 1978 | 42 | Febrile | No data | Peritoneal fluid, blood culture | Yes |
| 1978 | 65 | Febrile | No data | Peritoneal fluid | Yes | |
| Bannatyne3 | 1977 | 4 | Febrile | C | Peritoneal fluid | Yes |
| Weintraub13 | 1974 | 32 | Meningeal syndrome | C | CSF | No |
This table illustrates reported cases of meningococcemia presenting as acute abdomen in global literature since 1974. The table is divided into 7 vertical columns indicating reported case, year of publication, patient's age, clinical manifestation upon presentation, pathogen serotype, site of Neisseria isolation and whether surgery was carried out respectively.
CSF, cerebrospinal fluid.
Contrary to purulent pericarditis, RMP represents a late complication and very few cases have been reported in literature.1,15–19 It develops most frequently 6–15 days after onset of illness and is characterized by a type 3 hypersensitivity reaction, either against the specific serotype of the N. meningitidis or newly antigenic, damaged pericardial tissue because of molecular mimicry with microbial antigens.20 Severe disease, age (adults and young teenagers), and serogroup C seems to predispose to post-infectious immune associated complications including arthritis, vasculitis, pleuritis, or pericarditis.15,16,20 In line with these observations, our patient was a young adult, presenting in poor clinical condition, with highly elevated inflammatory markers suggestive of severe disease, even though interestingly serogroup B (and not C) was finally isolated. The pericardial fluid in RMP is serous and sterile, and is often associated with polyserositis not responsive to antibiotics but to NSAIDs.1,18 RMP may be more severe than purulent pericarditis and cardiac tamponade can be relatively frequent requiring high dosages of steroids and/or pericardiocentesis.20 Recurrent pericarditis is exceptionally rare after the meningococcal infection (Table 2), while the reasons of its recurrence remain unknown, even though genetic factors have been proposed.15–18 In these cases, the course of the disease may be chronic and unpredictable, regardless of the therapy given or the triggering cause, while corticosteroid use can induce severe dependence.
Cases of recurrent reactive meningococcal pericaditis in literature since 1969.
| Reference | Patient age | Time of pericarditis diagnosis | Site of isolation | Neisseria meningitidis serogroup | Clinical presentation | Therapy | Outcome |
|---|---|---|---|---|---|---|---|
| Chiappini15 | 10y/o | 7d | CSF | C | Meningitis | Prednisone+Aspirin | Recurrence |
| El Bashir16 | 13y/o | 7d | Blood | C | Meningitis | Dexamethasone +Ibuprofen, later diclofenac sodium | Recurrence |
| Dupont17 | 14y/o | 3d | CSF | C | Meningitis | ASA | Recurrence |
| Lanchemayer18 | 45y/o | 8d | CSF | No data | Meningitis | Hydrocortisone | Recurrence |
| Stange19a | No data | No data | CSF | B | No data | No data | Recurrence |
| 47y/o | 7d | CSF | No data | Meningitis | ASA+NSAID+Pericardiocentesis | Recurrence | |
| Stephani24 | 14y/o | 9d | CSF, blood | C | Meningitis, endopthalmitis | Prednisone+Antibiotics | Recurrence |
| Fuglsang Hansen25a | No data | 11d | No data | No data | Meningitis | Steroid+Pericardiocentesis | Recurrence |
This table illustrates reported cases of meningococcal recurrent reactive pericarditis in global literature since 1969 The table is divided into 8 vertical columns indicating reported case, patient's age, time of pericarditis diagnosis following onset of symptoms, site of Neisseria isolation, pathogen serotype, clinical manifestation upon initial presentation, therapeutic scheme and outcome respectively.
d, days; CSF, cerebrospinal fluid; ASA, acetylsalicylic acid; NSAID, non steroid anti inflammatory drug.
It would be intriguing to hypothesize that severe disease – commonly associated with higher antigenic loads – could have triggered overt immune complex formation and later deposition to abdominal vascular bed and pericardium, responsible for initial presentation and secondary complication respectively. Careful initial examination, close observation and high clinical suspicion may be required so that an atypical presentation, as well as, manifestation during the course of the disease is not overlooked, even after appropriate antibiotic treatment of meningococcal meningitis has occurred.
ConsentWritten informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Conflicts of interestThe auathors declare no conflicts of interest.
Authors’ contributionsKA performed literature review, wrote the manuscript and designed figure and tables. AA was the attending internal medicine resident, NK performed cardiologic assessments and consults and provided images. CG oversaw patient's management. AL critically corrected the manuscript and was the attending infectious diseases specialist.
