

Non-aneurysmal infectious aortitis is a rare clinical disease that is lethal when surgical intervention is delayed. Aeromonas species are common pathogens that cause gastrointestinal disorders; however, the extra-intestinal septic syndrome is rare.1,2 Extra-intestinal infections include empyema, meningitis, endocarditis, arthritis, and soft tissue infections.1-4 Herein, we present a case of Aeromonas bacteremic aortitis complicated by a ruptured mycotic aneurysm. A series of computerized tomography images illustrate the complete development of this disease (Figs. 1 A, B, and C). To the best of our knowledge, this is the first documented case of infectious aortitis caused by Aeromonas sobria bacteremia.
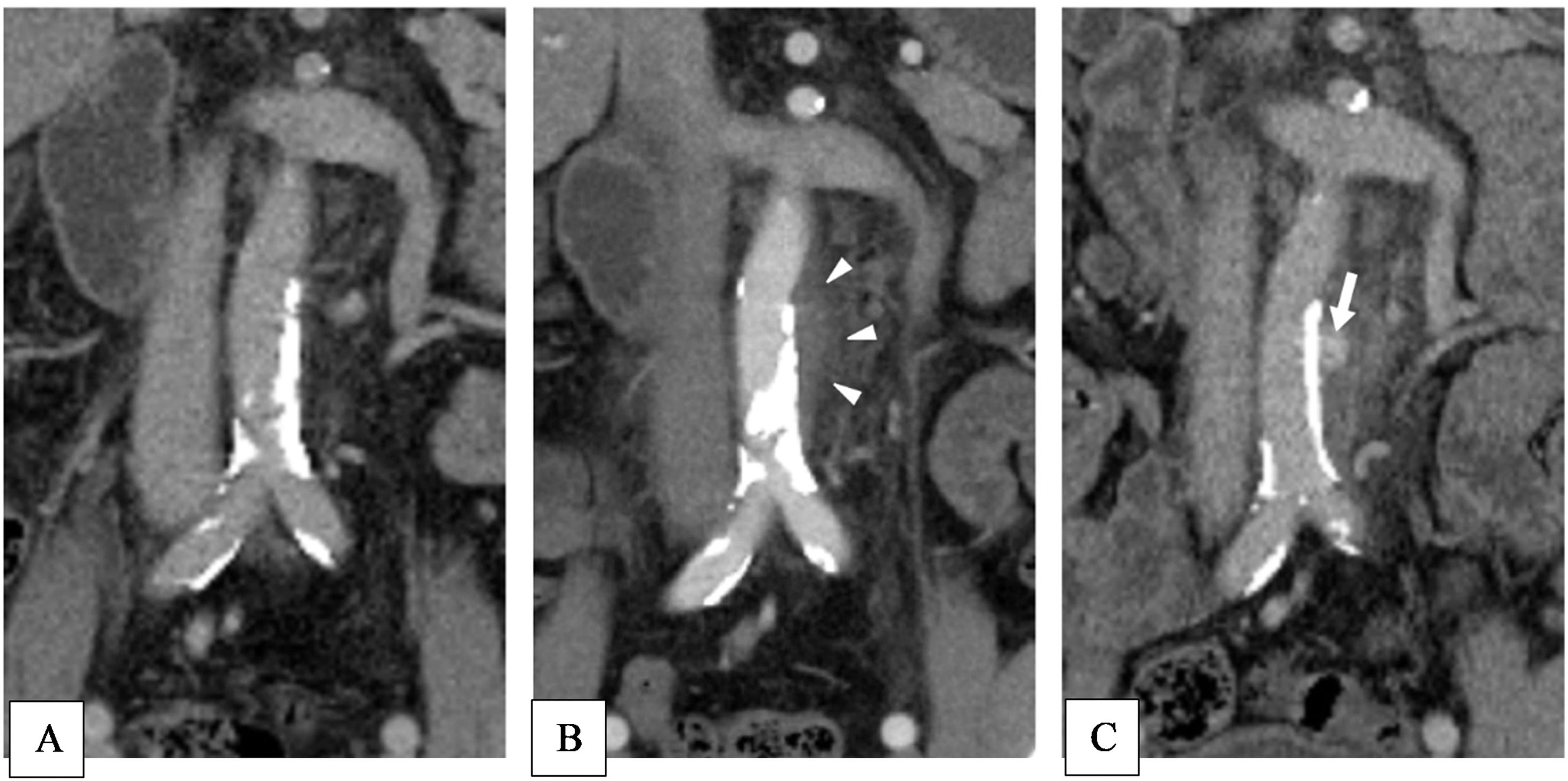
A 52-year-old man with liver cirrhosis presented to the emergency department with fever and abdominal pain. Laboratory data revealed leukocytosis and elevated C-reactive protein. Abdominal computerized tomography (Fig. 1A) revealed severe calcified atherosclerosis of the abdominal aorta. Empirical antibiotic therapy with cefuroxime (1.5 g) via an Intravenous drip (ivd) q8h was administered. Three days later, duplicate sets of blood cultures revealed Aeromonas sobria, which was sensitive to cefuroxime. The isolate (A. sobria) was analyzed by Matrix-Assisted Laser Desorption Ionization-time of Flight mass spectrometry (MALDI-TOF) using Bruker Biotyper (Bruker Daltonik GmbH, Bremen, Germany) and identified as A. sobria (score value, 2.18). In order to identify aeromonads at species level, a fragment of approximately 1100 bp of the gyrB gene from the isolate was amplified by PCR using primers GyrB3F and GyrB14R in a GeneAmp® PCR System 9700 thermal cycler (Applied biosystems, Foster city, CA, USA). Complete antibiotic therapy was administered for 14 days, and the patient was discharged. One month later, the abdominal pain relapsed. Additionally, severe backache was noted. Echocardiography revealed preserved left ventricular ejection fraction and no vegetation or valvular regurgitation. Again, the blood culture grew A. sobria. Hence, conservative treatment with parenteral ceftriaxone (2g) ivd qd was administered because the patient refused surgical intervention. The patient was free from clinical symptoms three days later, and parenteral ceftriaxone was prescribed for 21 days. Oral antibiotics with cefixime 500 mg bid were administered for two weeks after discharge.
However, the patient presented with similar symptoms three months later, including fever and backache. Abdominal CT revealed a mycotic aneurysm with contrast leakage at the level of previous aortitis (arrows, Figs. B and C). Based on the diagnosis of a ruptured mycotic aneurysm, emergent Endovascular Aneurysm Repair (EVAR) surgery was performed. The tissue culture of specimen of mycotic aneurysm also revealed A. sobria. Parenteral ceftriaxone (2g) ivd q12h was administered for eight weeks after surgery. After discharge from the hospital, oral ciprofloxacin 500 mg bid and rifampicin 600 mg qd were administered for another eight-week course. The patient was free from relapse even without the antibiotic treatment.
The genus Aeromonas is divided into two major groups: A. hydrophila, A. caviae, A. veronii, and A. sobria. Aeromonas septic syndrome is associated with immunocompromising conditions and contact with fresh water.1-4 In a case series study, the one-month mortality rate with Aeromonas bacteremia in patients with liver cirrhosis was 55%,2,4,5 especially in those who presented with an initial shock status and a history of malignancy.3,4
Infectious aortitis is a rare clinical condition that is most often associated with abdominal aortic atherosclerosis.1-4 Most infectious aortic aneurysms are of bacterial origin, among which Salmonella infection is the most common, followed by Staphylococcus aureus.1-5 To the best of our knowledge, there have been no documented cases of infectious aortitis or mycotic aneurysms caused by A. sobria infection.
Endovascular repair is a feasible therapeutic option for infectious aortitis because it can prevent the development of bleeding and rupture of aneurysms. In a case series of bacteremia caused by Aeromonas, most of the pathogens were not susceptible to ampicillin or first-generation cephalosporins; more than 90% of the clinical isolates were susceptible to third-generation cephalosporins, aminoglycosides, fluoroquinolones, and carbapenem.3-5 Establishing an accurate diagnosis of aortic infection before aneurysm formation and rupture is very difficult, but it is important in order to prevent devastating complications.3-5
In conclusion, although rare, Aeromonas sobria bacteremic aortitis may occur in immunocompromised patients with liver cirrhosis. Incomplete antibiotic treatment may cause recurrent bacteremia and mycotic aneurysm rupture. EVAR and prolonged antibiotic treatment are required in complicated cases.
Ethics approvalEthics approval was not required for this study and all authors consented to participate.
Consent for publicationThe patient consent and agree to publication.
Availability of supporting dataThe data from the electrical medical record of Taipei Municipal Wan Fang hospital.
Authors' contributionsKe-Shiuan Ju: collect the data and write manuscript. Wei-Ta Chen: concept of the figure. Ying-Shih Su and Wen-Sen Lee: correct the manuscript and English editing. All authors agree to publish this manuscript.
FundingNo funding support to this study.
