


Influenza viruses cause significant morbidity and mortality in both children and adults during local outbreaks or epidemics. Therefore, a rapid test for influenza A&B would be useful. This study was conducted to evaluate the clinical performance of the Wondfo influenza A&B test for rapid diagnosis of influenza A H1N1 Infection. The rapid testing assay could distinguish infection of influenza A and B virus. The reference viral strains were cultured in MDCK cells while TCID50 if the viruses were determined. The analytical sensitivity of the Wondfo kit was 100TCID50/ml. The Wondfo kit did not show cross reactivity with other common viruses. 1928 suspected cases of influenza A (H1N1) virus infection were analyzed in the Wondfo influenza A&B test and other commercially available products. Inconsistent results were further confirmed by virus isolation in cell culture. The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) were 100%, 98.23%, 92.45%, and 100% for flu A, and 96.39%, 99.95%, 98.77%, and 99.84% for flu B respectively. 766 suspected cases of influenza A (H1N1) virus infection were analyzed in the Wondfo influenza A&B test and RT-PCR. The sensitivity, specificity, PPV and NPV were 56.5%, 99.75%, 99.52% and 71.04% for flu A, 25.45%, 99.86%, 93.33% and 94.54% for flu B respectively. These results indicate that the Wondfo influenza A&B test has high positive and negative detection rates. One hundred fifty-six specimens of influenza A (H1N1) confirmed by RT-PCR were analyzed by the Wondfo influenza A&B test and 66.67% were positive while only 18.59% were positive by the reference kit. These results indicate that our rapid diagnostic assay may be useful for analyzing influenza A H1N1 infections in patient specimen.
Influenza, or flu, is an acute respiratory infection caused by a variety of influenza viruses. Influenza epidemics and pandemics can result in substantial health (clinical illness, hospitalization, deaths) and socioeconomic (absenteeism, decrease in productivity, decrease in travel and trade) impacts.1 A novel influenza A (H1N1) virus emerged in Mexico in early 2009 and then spread to more than 170 countries and regions.2 Influenza are highly infectious, mainly through coughing and sneezing and other respiratory pathways of communication. Influenza is a significant cause of morbidity and mortality, particularly in the young and elderly.3 According to the virus gene homology, there are three types of influenza virus, A, B and C. The influenza A's variation is the largest, and the most popular. Therefore, differentiation of influenza virus from other respiratory viruses is of prime importance because influenza is associated with higher rates of morbidity and mortality, is potentially preventable by vaccination, and can now be treated with specific antiviral drugs.4 Since the diagnosis of influenza can be difficult when based solely on clinical symptoms, rapid diagnosis of influenza permits the initiation of antiviral therapy within a beneficial time frame, can result in discontinuation of inappropriate antibiotics, and prompts infection control measures to reduce spread in healthcare settings.5–7
There are several different methods to diagnose influenza. The “gold standard” for diagnosis of influenza is tissue culture and virus isolation, which may take 2–14 days. Detection of virus-infected cells in nasopharyngeal secretions by direct or indirect immunofluorescent staining is widely used but is quite technique and technician dependent. In addition, it still requires at least 2h to finish.8 RT-PCR remains the method of choice for clinical diagnosis of S-OIV H1N1 virus in respiratory specimens and for differentiating it from seasonal influenza viruses.9 However, such tests are of high-complexity and cannot be readily performed in primary health care settings.10 The rapid influenza diagnostic test (RIDT), based on immunochromatographic lateral flow tests, is currently the best choice for screening samples for the diagnosis of influenza virus due to its rapid detection ability, simple operation and low cost. RIDT is unable to further classify influenza A virus subtypes and is not as sensitive as RT-PCR. However, it can provide a rapid diagnosis of influenza A or B infection to aid clinical management in half an hour.
In the present study we have investigated the clinical performance of the Wondfo influenza A&B test for their ability to detect and differentiate influenza A and B antigens. Furthermore, their analytical sensitivity, specificity and interfering factors were determined. The sensitivity, specificity and positive predictive value (PPV) and the negative predictive value (NPV) were compared with commercially rapid diagnostic kit, RT-PCR, and virus isolation in cell culture for detection of influenza H1N1 viral antigen in respiratory specimens collected during the 2009 pandemic period.
Materials and methodsSpecimen collectionThe virus strains used to evaluate Wondfo influenza A&B test included influenza A viruses A/14160 (H1N1), A/30 (H1N1), A/44045 (H3N2), A/924 (H3N2), avain influenza virus A/Beijing/302/54 (H5N1) and A/swine/Guangdong/2/01 (H1N1), influenza B viruses B/1715, B/1704, B/179, B/668, as well as other viruses, such as adenovirus, respiratory syncytial virus, herpes simplex virus type 1, herpes simplex virus type 2, rhinovirus type 2, parainfluenza virus type 2, parainfluenza virus type 3, mumps virus. They were obtained from the Center for Disease Control and Prevention of Guangdong Province. Mycoplasma pneumoniae, Chlamydia pneumoniae, and Mycobacterium tuberculosis were isolated at the Microbial Research Center within Sun Yat-Sen University. 156 influenza A (H1N1) specimens confirmed by RT-PCR were isolated in the Center for Disease Control and prevention of Guangdong Province. The 1928 suspected specimens of influenza A (H1N1) virus infection including 766 specimens detected by RT-PCR were collected during the 2009 pandemic period in the Center for Disease Control and prevention of Guangzhou, Guangzhou Women and Children Medical Center, Guangzhou No. 8 People's Hospital, People's Liberation Army No. 302 Hospital and Guangdong Entry-Exit Inspection and Quarantine Technology Center.
Analytical sensitivity, specificity and cross reactivityTen virus isolates of A/14160 (H1N1), A/30 (H1N1), A/44045 (H3N2), A/924 (H3N2), A/Beijing/302/54 (H5N1), A/swine/Guangdong/2/01 (H1N1), B/1715, B/1704, B/179, B/668 were cultured in Mardin Darby Canine Kidney (MDCK) cells. The culture supernatants were aliquoted and frozen at −80°C. They were evaluated to determine the limit of detection of the Wondfo flu A&B test (Wondfo Biotech Co., Ltd., Guangzhou, China). An aliquot of each virus was thawed and a series of 10-fold dilution prepared. The testing was carried out according to the manufacturer's instructions. Furthermore, a series of twofold dilutions were done in duplicate from the end point obtained above. The diluted virus isolates were used to infect MDCK cells to determine TCID50 of the virus. To determine the specificity and cross reactivity of the Wondfo influenza A&B fast test strip, commensal and pathogenic micro-organisms (influenza B virus, influenza A virus, respiratory syncytial virus, adenovirus, herpes simplex virus type 1, herpes simplex virus type 2, rhinovirus type 2, parainfluenza virus type 2, parainfluenza virus type 3, mumps virus, Mycoplasma pneumoniae, Chlamydia pneumoniae, Streptococcus pneumoniae, Mycobacterium tuberculosis) that may be present in the nasal cavity or nasopharynx were tested. Bacteria were cultured and suspended in sterile Dulbecco's phosphate buffered saline at concentrations of 108CFU/ml. Viral isolates were tested at titers between 103 and 108TCID50/ml.
Comparison of characteristic of Wondfo test and reference kitOne thousand nine hundred twenty-eight suspected cases of influenza A (H1N1) virus infection were tested by Wondfo influenza A&B kit and other commercially kit (Hangzhou Genesis Biodetection & Biocontrol Ltd., called as GENESIS) as reference kit. The specimens with inconsistent results in the above testing were further confirmed by virus isolation in cell culture. The result is positive detected by the both kits or the result is positive detected by one kit and is confirmed positive by virus isolation in cell culture. Other results, not positive, are true negative. The sensitivity, specificity, PPV and NPV of Wondfo kit were calculated.
Comparison of characteristic of RDTs and RT-PCRSeven hundred sixty-six suspected cases of influenza A (H1N1) virus infection were tested by two rapid diagnostic tests (RDTs, Wondfo influenza A&B Kit and GENESIS kit) with RT-PCR (UT-BIOMED International, Canada) as the reference method. Sensitivity and predictive values were determined and the differences of sensitivity and predictive values were compared between RDTs and RT-PCR.
Comparison of detection rate of H1N1 of Wondfo kit and reference kitOne hundred fifty-six cases of H1N1 virus infection collected during the influenza epidemic in 2009 were confirmed by RT-PCR by Center for Disease Control and Prevention of Guangdong Province. The testing results of Wondfo influenza A&B kit were compared with other commercially kit (GENESIS) as reference kit.
ResultsAnalytical sensitivity, specificity and cross reactivityThe estimated limit of detection for the 10 influenza virus isolates was summarized in Table 1. It can be seen that the Wondfo test could detect as low as 1.7×103TCID50/ml of influenza A virus and 6.3×102TCID50/ml of influenza B virus. The results indicated that the Wondfo influenza A&B test could distinguish infection of influenza A and B virus, but did not show cross reactivity with non-influenza viruses that we tested.
Comparison of characteristic of Wondfo and reference kitTable 1 shows the results of 1928 specimens detected by two rapid diagnostic test kits and compare results with virus isolation in cell culture as the gold standard. The sensitivity, specificity, PPV and NPV of Wondfo influenza A&B were 100%, 98.23%, 92.45%, and 100% for fluA, respectively and 96.39%, 99.95%, 98.77%, and 99.84% for flu B, respectively. The sensitivity, specificity, PPV and NPV of GENESIS were 71.72%, 99.30%, 95.72%, and 94.20% for flu A, and 98.80%, 99.84%, 95.35%, and 99.95% for flu B respectively. For flu A, the sensitivity of the Wondfo kit was greater than that of GENESIS, but for flu B, the two methods had no significant difference.
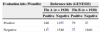
Comparison of characteristic of RDTs and RT-PCRTable 2 shows the results of 766 specimens detected by two rapid diagnostic test kits and compare results with RT-PCR method. It can be concluded that the sensitivity, specificity, PPV and NPV of Wondfo influenza A&B were 56.5%, 99.75%, 99.52%, and 71.04% for flu A, respectively and 25.45%, 99.86%, 93.33%, and 94.54% for flu B, respectively. The sensitivity, specificity, PPV and NPV of GENESIS were 31.62%, 98.74%, 95.90%, and 60.71% for flu A, and 23.64%, 99.72%, 86.67%, and 94.41% for flu B respectively. For flu A, the sensitivity of the Wondfo kit was greater than that of GENESIS, but for flu B, the two methods had no significant difference. The sensitivity was greater for the Wondfo kit (56.50%) than GENESIS (31.62%) in detecting flu A. The sensitivity was similar for the Wondfo kit (25.45%) than GENESIS (23.64%) in detecting flu B. The specificity, PPV and NPV of both Wondfo influenza A&B test and the reference influenza tests were consistent.
Results of the Wondfo influenza A&B test, GENESIS and RT-PCR in detection of clinical specimens suspected influenza A (H1N1) virus infection (n=766).
| RT-PCR | ||||
|---|---|---|---|---|
| Flu A (n=766) | Flu B (n=766) | |||
| Positive | Negative | Positive | Negative | |
| Evaluation reagents (Wondfo) | ||||
| Positive | 209 | 1 | 14 | 1 |
| Negative | 161 | 395 | 41 | 710 |
| Reference reagents (GENESIS) | ||||
| Positive | 117 | 5 | 13 | 2 |
| Negative | 253 | 391 | 42 | 709 |
The 156 influenza A (H1N1) specimens were confirmed by RT-PCR. The results are shown in Table 3. It can be concluded that 66.67% (104/156) were positive by Wondfo influenza A&B test while only 18.59% (29/156) were positive by the GENESIS kit.
DiscussionAlthough the gold standard for detecting influenza virus infection is virus isolation in cell culture, it takes too long to get results, which in turn would delay the action to initiate antiviral treatment and to take measures to prevent flu epidemic and transmission. Therefore, rapid tests in a time of minutes are definitely necessary.
The Wondfo influenza A&B test used in our study has been previously shown to be effective in detecting seasonal influenza viruses.10 The test was able to specifically detect all influenza viruses (type A and B) including H1N1, H3N2, H5N1 virus (Table 1). The analytical sensitivity (detection limit range: 6.3×102–3.2×107TCID50/ml) of the flu A&B test was established for seven flu A and four flu B isolates. For the cross reactivity study, none of the 14 microorganisms tested (bacteria and viruses) turned out positive by the Wondfo influenza A&B fast test, indicating very good specificity.
Our results show that the sensitivity was greater for the Wondfo kit than other commercially available kits in detecting flu A. Compared with other commercially available kits, the sensitivity of the Wondfo influenza A&B fast test was 100% for influenza virus A and 96.36% for influenza virus B for flu A. The results of the two methods had significant difference (p<0.05) and the two RIDT reagents were common consistent results (Kappa=0.743, p=0.021, p<0.05). Compared with RT-PCR assay, the sensitivity of the Wondfo influenza A&B fast test for influenza virus A was also much higher than that of other commercially available kits. The high sensitivity of Wondfo test for influenza A was confirmed by testing 156 influenza A (H1N1) specimens that were confirmed by RT-PCR. The positive detection rate of the Wondfo influenza A&B test for H1N1 was 66.67%. However, with the other commercially available kit it was 18.59%. These results suggested a better performance of the Wondfo influenza A&B fast test than that of the other commercially available kits used in our study.
Conflict of interestAll authors declare to have no conflict of interest.
We express our thanks to Prof. Shujuan Yu and Dr. Shixing Tang for their excellent technical help and critical comments.
