
The human retroviruses HIV-1 and HTLV-1 share the routes of infection with hepatitis viruses B and C. Co-infection by these agents are a common event, but we have scarce knowledge on co-infection by two or more of these agents.
ObjectiveTo evaluate the characteristics and risk factors for co-infections by HBV and HCV in patients infected by HIV-1 or/and HTLV-1, in Salvador, Brazil.
MethodsIn a case–control study we evaluated patients followed in the AIDS and HTLV clinics of Federal University of Bahia Hospital. Clinical and epidemiological characteristics were reviewed, and patients were tested for the presence of serological markers of HBV and HCV infections. HCV-infected patients were tested by PCR to evaluate the presence of viremia.
ResultsA total of 200 HIV-1, 213 HTLV-1-infected, and 38 HIV-HTLV-co-infected individuals were included. HIV-infected patients were more likely to have had more sexual partners in the lifetime than other patients’ groups. HIV-HTLV-co-infected subjects were predominantly male. Patients infected by HTLV or co-infected had a significantly higher frequency of previous syphilis or gonorrhea, while HIV infection was mainly associated with HPV infection. Co-infection was significantly associated to intravenous drug use (IVDU). HBV and/or HCV markers were more frequently found among co-infected patients. HBV markers were more frequently detected among HIV-infected patients, while HCV was clearly associated with IVDU across all groups. AgHBs was strongly associated with co-infection by HIV-HTLV (OR=22.03, 95% CI: 2.69–469.7), as well as confirmed HCV infection (p=0.001). Concomitant HCV and HBV infection was also associated with retroviral co-infection. Patients infected by HTLV-1 had a lower chance of detectable HCV viremia (OR=0.04, 95% CI: 0.002–0.85).
ConclusionsInfection by HCV and/or HBV is frequent among patients presenting retroviral infection, but risk factors and prevalence for each infection are distinct for each agent. Retroviral co-infection increases the risk of a positive AgHBs, but HTLV-1 infection seems to increase the likelihood of HCV spontaneous clearance.
Viral hepatitis are important health problems worldwide.1–4 It is well known that simultaneous infection by HIV-1 and the viruses of hepatitis B or C can modify the outcomes of such infections, with a higher likelihood of chronic liver disease, and a greater risk of rapid evolution to liver fibrosis.5 The introduction of highly active antiretroviral therapy as standard of care for AIDS treatment increased the life expectancy of HIV-1-infected patients, and chronic liver disease became a common finding and a leading cause of death among co-infected patients.6,7
Although the natural history of co-infection by HIV-1 and viral hepatitis B (HBV) and C (HCV) is well known, there is scarce data on the characteristics and clinical impact of co-infection by HBV or HCV and another human retrovirus, the human T-cell lymphotropic virus type-1 (HTLV-1). HTLV-1 shares the same route of infection that are commonly associated with HIV-1 infection.8 However, the biological characteristics of these viruses are quite distinct, making the outcome of co-infection by these agents unpredictable. In a recent work, we demonstrate that patients co-infected by HIV-1, HTLV-1 and HCV had a lower chance to present liver fibrosis than those co-infected only by HCV and HIV-1, suggesting a potential protective role of HTLV-1.9 Since co-infection by HIV-1 and HTLV-1 is a frequent finding is some areas of the world, it is important to evaluate the risk factors for simultaneous infection by human retroviruses and HBV/HCV. Our goal in the present work was to describe the epidemiological characteristics of patients co-infected by HIV-1, and/r HTLV-1, HCV and HBV.
MethodsStudy designThis is a case–control study to compare the risk factors for co-infection by viral hepatitis B (HBV) and C (HCV) among Brazilian patients infected by HIV-1 (cases), HTLV-1, or both retroviruses (controls).
Patients and settingsHIV-infected patients (case group): a total of 200 consecutive HIV-positive patients during their regular visit to clinical follow-up or laboratory evaluation entered the study. The entry criteria were: a Western blot (WB) confirmed infection by HIV-1, a negative serology for HTLV-1 and age≥18 years.
HTLV-1 infected patients (control group 1): a total of 213 consecutive patients were included in the study. WB confirmed infection by HTLV-1, and a negative serology for HIV-1 and age≥18 years.
HIV-1-HTLV-1 co-infected group (control group 2): a total of 38 HIV-infected patients (older than 18 years) with a simultaneous positive serology for HTLV-1.
All patients were recruited in HIV or HTLV outpatients’ clinics of Federal University of Bahia Hospital, and provided a written informed consent to enter the study, which was approved by the institutional ethics review board (IRB). They were interviewed and had their medical charts reviewed to collect information on gender, age, sexual behavior (sexual orientation, number of current/lifetime sexual partners, and previous history of sexually transmitted diseases), and illicit drug use.
Sample size calculationAround 2500 HIV-infected patients are followed in our AIDS clinic, while the HTLV clinic cares for approximately 600 patients. We calculated the sample size to have a power of 80% and a 95% confidence interval (CI), by using an expected prevalence of HBV equal to 5.5% for HIV-infected individuals and an infection rate similar to that found in general population (0.5%) for HTLV-infected subjects. This would require 197 patients in each group. For HCV, using the estimated rate of 3% of infection for general population and 15% for HIV-infected individuals we would need 167 patients in each group. For co-infected patients we estimated a 40% prevalence of HCV infection, which would result in a sample of 23 patients in this group. For HBV infection, using an estimate of 25% prevalence we would need 26 individuals to have the same power and CI. All co-infected cases under regular follow-up in our clinics were included.
Laboratory testsSerological screening for HIV-1 and HTLV-1As a routine in our service, HIV infected patients are screened by enzyme immunoassays (EIA) for HTLV-1/2 antibodies (Vironostika or Murex). Reactive samples are confirmed by a Western blot (Wb) test, capable of discriminating between HTLV-1 and HTLV-2 infections (Genelabs, Singapore). Similarly, all HTLV-1 patients are routinely screened for HIV-1 antibodies by EIA. HIV-1 infection confirmation is made by Wb or by molecular methods (viral load determination by NASBA until 2007 and b-DNA from 2007 to present). Screening tests for both retroviruses were acquired from different licensed manufacturers, since the serological diagnosis for both infections in our study covered several years, and patients were evaluated in different periods of time. All patients included in the study were asked to provide a blood sample for laboratory tests. Plasma samples were stored at −20°C until further testing.
Hepatitis B (HBV) and C (HCV) infectionAll patients were tested for markers of HBV infection (AgHBs and Anti-HBc serology) by EIA (Diasorin, Vercelli, Italy). Anti-HCV antibodies were detected by EIA (Diasorin, Vercelli, Italy) and reactive samples were confirmed by RIBA (Chiron RIBA HCV 3.0 Strip Immunoblot Assay). Detection of HCV in plasma was attempted by RT-PCR (EZ r Tth RNA PCR Kit, Applied Biosystems) in a single step, using the primers of the non-codifying region 5′ KY 78 CAC TCG CAA GCA TAT CAG GCA GT, and KY 80 GCA GAA AGC GTG TAG CCA TGG CG.
Patients presenting with HCV detectable viremia had their genotypes determined by TruGene sequencing system (TRUGENE 5′NC – Visible Genetics Toronto – Canadá – Bayer Health Care Diagnostics).
Statistical analysisOur main outcomes of interest were markers of risk exposure to HIV-1, HTLV-1 and HCV/HBV infections. We calculated prevalence and 95% confidence intervals (CI) based on binomial distributions. Summary statistics included frequency tables for categorical variables, medians and interquartile range (IQRs) for continuous variables. We conducted univariate analyses examining associations between groups using the chi-square test, or Fisher's exact test (when appropriate), and calculated odds ratios (ORs) and 95% confidence intervals (CI). To further examine associations in subgroups of interest, in particular between risk factors for different infections, we conducted stratified analyses.
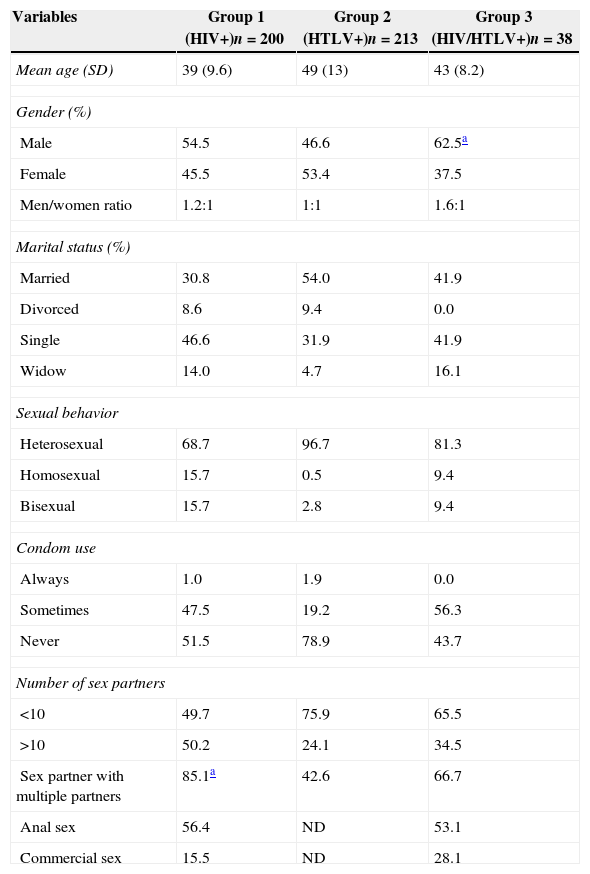
ResultsDemographics and risk behavior for acquisition of infectionsThe mean age was similar for the three groups, but patients in co-infected (HIV-HTLV) group were significantly more likely to be male (p=0.001, Yates corrected). Although it did not reach statistical significance, we observed a higher frequency (31%) of men reporting sex with other men (MSM) in group 1, than in group 2 (3%) or group 3 (19%). The use of condoms was seldom reported: almost all patients (98%) in the 3 groups declared not to use condoms during sexual intercourse. A significant difference was detected in the number of sexual partners (lifetime) across the groups: 50% of patients in group 1 (HIV-1-infected) reported more than 10 sexual partners, in comparison with 24% of those in group 2 (HTLV-1 infection), and 34.5% in group 3 (p<0.001 for comparison between group 1 and groups 2 or 3). On the other hand, a significant difference (p<0.01) was found in the frequency of illicit drug use (IDU), with patients in Group 1 (16.2%), and Group 2 (3%) reporting a significantly lower frequency of IDU, in comparison with those in Group 3 (32%, p<0.01, Yates corrected). Table 1 shows the main characteristics of the patients involved in the study. In addition, significantly more patients in group 1 reported IVDU as sexual partners, compared with only 8% of those in group 2 (p=0.001, Yates corrected). Among co-infected patients, 32% declared themselves to be illicit drug users (90% IV), and 46% had an IVDU sexual partner (p=0.001 compared with group 2). The history of previous use of blood or blood products was not significantly different in group 1 (8%), group 2 (19%) and group 3 (15%). The frequency of patients who were breastfed was similar in groups 2 (88%) and 3 (98%). For group 1, this information was unavailable.
Demographic characteristics of patients and risk factors for acquisition of retroviral infection, according to their serological status for HIV and HTLV.
| Variables | Group 1 (HIV+)n=200 | Group 2 (HTLV+)n=213 | Group 3 (HIV/HTLV+)n=38 |
|---|---|---|---|
| Mean age (SD) | 39 (9.6) | 49 (13) | 43 (8.2) |
| Gender (%) | |||
| Male | 54.5 | 46.6 | 62.5a |
| Female | 45.5 | 53.4 | 37.5 |
| Men/women ratio | 1.2:1 | 1:1 | 1.6:1 |
| Marital status (%) | |||
| Married | 30.8 | 54.0 | 41.9 |
| Divorced | 8.6 | 9.4 | 0.0 |
| Single | 46.6 | 31.9 | 41.9 |
| Widow | 14.0 | 4.7 | 16.1 |
| Sexual behavior | |||
| Heterosexual | 68.7 | 96.7 | 81.3 |
| Homosexual | 15.7 | 0.5 | 9.4 |
| Bisexual | 15.7 | 2.8 | 9.4 |
| Condom use | |||
| Always | 1.0 | 1.9 | 0.0 |
| Sometimes | 47.5 | 19.2 | 56.3 |
| Never | 51.5 | 78.9 | 43.7 |
| Number of sex partners | |||
| <10 | 49.7 | 75.9 | 65.5 |
| >10 | 50.2 | 24.1 | 34.5 |
| Sex partner with multiple partners | 85.1a | 42.6 | 66.7 |
| Anal sex | 56.4 | ND | 53.1 |
| Commercial sex | 15.5 | ND | 28.1 |
ND, unavailable data.
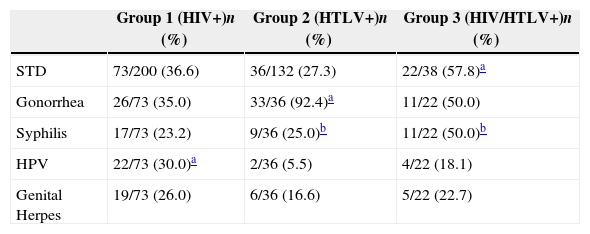
History of a previous sexually transmitted disease (STD) was significantly more frequent (p<0.001, Yates corrected) for patients in group 3 (58%) than for those in group 2 (27%) or group 1 (37%). The frequency of specific STDs was also different for each group. Group 1 were more likely to have a previous history of HPV (30%) than groups 2 (17%) or 3 (23%, p<0.001, Yates corrected), while group 2 reported more gonorrhea (92%) and syphilis (25%), and group 3 reported a higher frequency of syphilis (50%) than the other 2 groups (p<0.001 for all calculations). Table 2 shows the frequency of each STD for the different groups of patients.
Frequency of previous sexually transmitted diseases (STD) among the studied groups of patients.
| Group 1 (HIV+)n (%) | Group 2 (HTLV+)n (%) | Group 3 (HIV/HTLV+)n (%) | |
|---|---|---|---|
| STD | 73/200 (36.6) | 36/132 (27.3) | 22/38 (57.8)a |
| Gonorrhea | 26/73 (35.0) | 33/36 (92.4)a | 11/22 (50.0) |
| Syphilis | 17/73 (23.2) | 9/36 (25.0)b | 11/22 (50.0)b |
| HPV | 22/73 (30.0)a | 2/36 (5.5) | 4/22 (18.1) |
| Genital Herpes | 19/73 (26.0) | 6/36 (16.6) | 5/22 (22.7) |
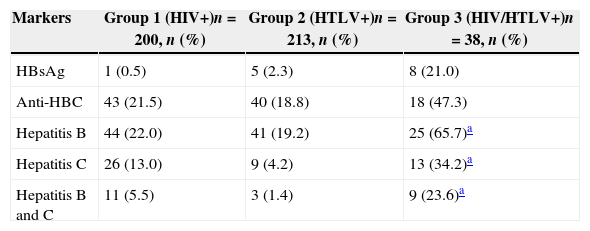
The overall frequency of serological markers for previous HBV infection (HBsAg and/or Anti-HBc) was 27.5% (55/200) in Group 1, 20.6% (44/213) in Group 2, and 89.5% (34/38) in Group 3 (p=0.001, Yates corrected). The prevalence of HBV surface antigen (HBsAg) was lower (0.5%) among HIV singly infected, and among HTLV-1-infected patients (2.5%), than in patients co-infected by both retroviruses (21.0%, OR=22.03, 95% CI: 2.69–469.7, p=0.0002, Yates corrected). The prevalence of anti-HCV (RIBA confirmed) was also higher among co-infected patients (28.9%), than in patients infected by HIV-1 alone (10.5%), or HTLV-1 alone (4.2%, p=0.001, Yates corrected). In addition, evidence of previous infections by both, HCV and HBV was also higher in the co-infected group (23.6%) than in singly infected by HIV-1 (5.5%) or HTLV-1 (1.4%, p<0.001, Yates corrected) groups. Table 3 summarizes the serological evidence for these infections.
Prevalence of serological markers for viral hepatitis B and C.
The risk factors associated with HCV and HBV infections were distinct for each group of patients: individuals with a positive marker for HBV were more likely to be male and infected by HIV-1 (70.5%), or co-infected by HIV-1 and HTLV-1 (78.0%), than HTLV-1-singly infected ones (58.5%, p<0.001, Yates corrected). In addition, patients infected by HIV-1 were more likely to be homo-bisexual than those infected by HTLV-1 alone (p<0.001, Yates corrected). HCV infection was basically associated with IVDU, for all groups of patients (p<0.01, Yates corrected, for all comparisons between groups).
The prevalence of detectable HCV RNA plasma viremia was compared in the three groups. Among patients with a RIBA-confirmed HCV infection, detectable HCV viremia was present in 17/17 (100%) samples tested among HIV-1 singly infected patients, in 4/7 (57.1%) of HTLV-1-infected patients, and in 8/11 (72.7%) of HIV-HTLV co-infected patients. Patients singly infected by HTLV-1 had a significantly lower likelihood of having detectable HCV viremia, in comparison with those infected by HIV-1 alone (singly or co-infected with HTLV-1, OR=0.04, 95% CI: 0.002–0.85).
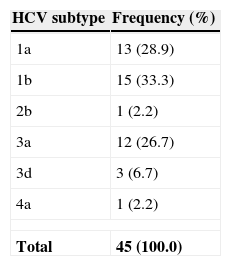
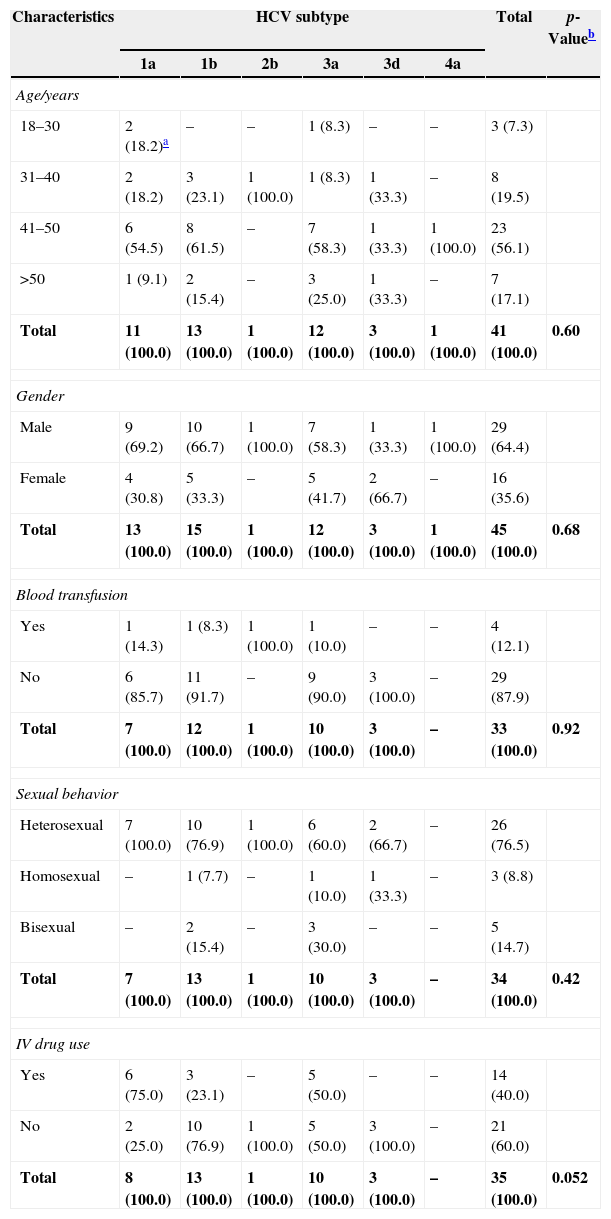
The distribution of HCV subtypes is presented in Table 4. We did not detect any association between specific HCV subtypes and co-infections, but there was a trend for higher frequency of subtype 1a among IVDU patients (Table 5).
Frequency of HCV subtypes among selected patients.a
| HCV subtype | Frequency (%) |
|---|---|
| 1a | 13 (28.9) |
| 1b | 15 (33.3) |
| 2b | 1 (2.2) |
| 3a | 12 (26.7) |
| 3d | 3 (6.7) |
| 4a | 1 (2.2) |
| Total | 45 (100.0) |
Demographic characteristics and risk factors for HCV infection according to HCV subtype.
| Characteristics | HCV subtype | Total | p-Valueb | |||||
|---|---|---|---|---|---|---|---|---|
| 1a | 1b | 2b | 3a | 3d | 4a | |||
| Age/years | ||||||||
| 18–30 | 2 (18.2)a | – | – | 1 (8.3) | – | – | 3 (7.3) | |
| 31–40 | 2 (18.2) | 3 (23.1) | 1 (100.0) | 1 (8.3) | 1 (33.3) | – | 8 (19.5) | |
| 41–50 | 6 (54.5) | 8 (61.5) | – | 7 (58.3) | 1 (33.3) | 1 (100.0) | 23 (56.1) | |
| >50 | 1 (9.1) | 2 (15.4) | – | 3 (25.0) | 1 (33.3) | – | 7 (17.1) | |
| Total | 11 (100.0) | 13 (100.0) | 1 (100.0) | 12 (100.0) | 3 (100.0) | 1 (100.0) | 41 (100.0) | 0.60 |
| Gender | ||||||||
| Male | 9 (69.2) | 10 (66.7) | 1 (100.0) | 7 (58.3) | 1 (33.3) | 1 (100.0) | 29 (64.4) | |
| Female | 4 (30.8) | 5 (33.3) | – | 5 (41.7) | 2 (66.7) | – | 16 (35.6) | |
| Total | 13 (100.0) | 15 (100.0) | 1 (100.0) | 12 (100.0) | 3 (100.0) | 1 (100.0) | 45 (100.0) | 0.68 |
| Blood transfusion | ||||||||
| Yes | 1 (14.3) | 1 (8.3) | 1 (100.0) | 1 (10.0) | – | – | 4 (12.1) | |
| No | 6 (85.7) | 11 (91.7) | – | 9 (90.0) | 3 (100.0) | – | 29 (87.9) | |
| Total | 7 (100.0) | 12 (100.0) | 1 (100.0) | 10 (100.0) | 3 (100.0) | – | 33 (100.0) | 0.92 |
| Sexual behavior | ||||||||
| Heterosexual | 7 (100.0) | 10 (76.9) | 1 (100.0) | 6 (60.0) | 2 (66.7) | – | 26 (76.5) | |
| Homosexual | – | 1 (7.7) | – | 1 (10.0) | 1 (33.3) | – | 3 (8.8) | |
| Bisexual | – | 2 (15.4) | – | 3 (30.0) | – | – | 5 (14.7) | |
| Total | 7 (100.0) | 13 (100.0) | 1 (100.0) | 10 (100.0) | 3 (100.0) | – | 34 (100.0) | 0.42 |
| IV drug use | ||||||||
| Yes | 6 (75.0) | 3 (23.1) | – | 5 (50.0) | – | – | 14 (40.0) | |
| No | 2 (25.0) | 10 (76.9) | 1 (100.0) | 5 (50.0) | 3 (100.0) | – | 21 (60.0) | |
| Total | 8 (100.0) | 13 (100.0) | 1 (100.0) | 10 (100.0) | 3 (100.0) | – | 35 (100.0) | 0.052 |
Our results demonstrated that, although HIV-1, HTLV-1, HCV, and HBV share some common routes of infection, the risks for acquiring these agents are quite distinct. HIV-1, as expected, was associated with a higher number of sexual partners, a higher likelihood of being male, homosexual, having an IVDU sexual partner, and having a higher number of sexual partners. Co-infection by HIV-1 and HTLV-1 was clearly associated with use of illicit drugs, especially by IV route, and with having IVDU as sexual partners. For group 2 (HTLV-1 infected patients) the only detected risk was a higher frequency of gonorrhea and syphilis.
There is clear association between a higher number of sexual partners and increased risk for HIV-1 infection. In addition, the association of sexual contact with IVDU and HIV-1 infection was also expected, since these patients usually present a risky behavior, through sharing injection equipment, having commercial sex, or sexual relationships with other high risk individuals.10,11 The detected linkage between specific STDs and HTLV-1 infection suggest a higher sexual exposure to HTLV-1, which seems to be the preferential route of transmission for this specific group.
The viral hepatitis agents HBV and HCV were much more prevalent across the study groups than in general population. Available data show that HCV (1–2%) and HBV (0.3–1%) are less frequent in the general population than that found in groups 1 and 3.12–15 However, the prevalence of HBsAg (an evidence of persistent HBV infection), was significantly lower in HIV-infected patients (0.5%) than in HTLV-1 (2.5%) or co-infected patients (21%) groups. It suggests that infection by HTLV-1 can reduce the spontaneous clearance of HBV, and this risk increases in the simultaneous presence of HIV-1 infection. In addition, HIV-1-HTLV-1 co-infected patients were also more likely (28.9%) to be also infected by HCV, than HIV-1 (10.5%) or HTLV-1 (4.2%) singly infected groups. Infection by both HBV and HCV were also more frequent in group 3, probably as a reflex of a higher prevalence of IVDU in this specific group.
The variables associated with HBV infection were being male, homo-bisexual, and infected by HIV-1. On the other hand, HCV infection was basically associated with IVDU. However, HCV spontaneous clearance was significantly less frequent for patients infected by HIV-1 than for those infected by HTLV-1 (singly or co-infected). This suggests that the interactions between these hepatotropic viruses and the two distinct human retrorviruses can be diverse: while HBsAg was less frequently found in HIV-1 infected patients, HCV viremia was more frequent in this group. On the other hand, co-infection by HTLV-1 seems to increase the spontaneous clearance of HCV viremia, but was associated with a higher rate of HBV antigenemia.
HTLV-1 infection has a controversial effect on HIV-1 infection natural course. Although it seems evident that HTLV-2 do not interfere in AIDS clinical course, several evidence of laboratory and clinical studies demonstrate that such interaction can be deleterious for HIV-1 infection.16–18 However, in a recent study we found that HTLV-1 can modulate the immune response of HIV-HTLV co-infected patients with an increase in the production of IL-2 and gamma-Interferon (Th1 type response).19 This fact could favor the immune response against HCV, which is largely dependent on endogenous production of interferon, providing the conditions for higher spontaneous clearance of HCV viremia. Our findings suggest that spontaneous HCV clearance is significantly more likely to occur in HTLV-1 infected patients, probably as a consequence of such immune modulation. A previous work conducted by our group had found similar results.9
On the other hand, the role of HIV-HTLV co-infection on HBV infection natural course is not well understood. As far as we could see, there is only a few epidemiological published papers on such co-infection, with low prevalence of simultaneous infections, but no information on the potential effects of HTLV on HIV-HBV infection natural history.4,20–22 Other confounding factor is the prevalence of simultaneous infection by all these four viral agents, in a limited number of patients, making difficult to clarify the exact role of each virus on these findings.
It came as a surprise to detect higher frequency of HBsAg in HTLV-1, and among HIV-HTLV-infected patients. This fact can suggest that HTLV-1 can negatively impact the HBV clearance (in contrast to that detected for HCV), and co-infection by HIV-1 can even amplify this effect. Again, the main limitations of our conclusions are the small sample size, which makes it difficult to clearly identify potential confounders.
Simultaneous HIV-1 and HTLV-1 infections are frequently detected in regions were these agents are prevalent. HCV and HBV also share some routes of transmission, which makes co-infection by all these agents quite a predictable finding, especially among IVDU. It is important to be aware of these potential interactions between such agents, since they can significantly affect the natural course of each of these viral infections, mostly for HIV-1 infected patients. Studies including a higher number of patients are necessary to better clarify these questions.
Conflicts of interestThe authors declare no conflicts of interest.
