
The aim of this study was to evaluate self-reported syphilis and associated factors in sexually active young adults (16–25 years old) in the Public Health System in Brazil. This was a cross-sectional study with 8071 participants recruited from 119 primary care units. Of these, 224 (2.86%, 95% CI 2.29–3.43%) reported having the disease. Age, lower socio-economic class, being a smoker, not using a condom at first sexual intercourse, and ever had a same-sex sexual experience were associated with syphilis. The results reinforce the importance of implementing strategies focused on socio-economic class and early sexual education that encourage condom use from the beginning of sexual activity.
The number of cases of syphilis are increasing in many countries and have reached the highest levels since the 1950s.1 Health agencies are alert for increases in the rate of syphilis diagnoses. In 2016, the World Health Organization adopted the Global Health Sector Strategy on Sexually Transmitted Infections,2 and Brazil declared syphilis to be an epidemic.
The young population is in a period of exploration in relationships and sexual behavior, which increases the probability of sexually transmitted infections (STI).3 Syphilis in reproductive-aged women is particularly troubling because of its potential for mother-to-child transmission during pregnancy, with dramatic adverse pregnancy outcomes. Furthermore, every new syphilis case represents a serious infection with the potential for problematic health outcomes, such as the possibility of enhanced HIV transmission or neurosyphilis.4
The majority of studies of syphilis are geographically restricted and/or focus on specific groups of individuals (HIV-infected, pregnant, or immunosuppressed patients), leading to selection bias.5 This study is the first nationwide study to evaluate self-reported syphilis and associated factors in sexually active young adults (16–25 years old) in the Public Health System in Brazil
This is a cross-sectional, nationwide, multicenter study planned to evaluate the prevalence of human papillomavirus and other STI, including syphilis.6 Participants were recruited in all 26 Brazilian capitals and the Federal District of Brasilia across the five geographical regions, between September 2016 and November 2017. Primary health care professionals were trained to acquire data by the central study coordinator. Participants were recruited from 119 public primary care units using the following different approaches: (i) eligible individuals who came to the unit for any reason were asked to participate; (ii) community health agents extended personal invitations; and (iii) nurses in school-based health promotion programs also extended invitations. The primary care units in each city were selected based on their representativeness of the health districts.
Criteria exclusion were pregnant women, those who delivered a baby in the last three months, those who have undergone a hysterectomy or trachelectomy, and those who have ever had cervical intraepithelial neoplasia grade 2 or higher.
All individuals answered a validated standardized questionnaire. The Brazilian Criteria of Economic Classification was used to analyze the socio-economic class, because this is a pricing classification system of the Brazilian public that divides the market exclusively in terms of economic classes based on ownership of assets.7 To evaluate alcohol and drug consumption habits, we asked about the use of these substances throughout life. We also asked about the number of sexual partners in the last year, current condom use (“When you have sexual relations, do you use a condom?”) and in the first sexual intercourse. To diagnose syphilis, we asked the participants if they had ever been diagnosed with some STI. Individuals who reported having STI were asked which infections, including an option of syphilis (current or in the past). Those who referred syphilis were considered positive. Unanswered questions were considered missing values.
The study was approved by the local research and ethics committees (number 1607032) and by the committees of the 27 cities. All participants provided written consent after being informed about the content of the study.
The data are described as mean and confidence intervals, frequency or absolute number. To compare proportions, a Chi-square test was used. Student’s t-test was used to compare continuous variables. Variables associated with self-reported syphilis were investigated through construction of a Poisson regression model with robust variance. For the multivariate analyses, a theoretical framework was structured with the variables associated with HPV infection, discriminating in hierarchical blocks. In the first model, socio-demographic and socio-economic characteristics were included. In the second model, smoking, alcohol consumption, and drug use were added to Model 1. In the full model, variables of sexual behavior were included to Model 2. The interaction between homosexual relationship and socio-economic class was analyzed to verify if homosexual could be an effect modifier due to the difference in prevalence of syphilis through these groups.
The sample size was purposely equal in all regions to maximize the diversity in less-populated areas. To adjust the distribution of the sample to the study population, we weighted the measures by population size in each capital and by sex.
The analyses were performed using the SAS software (Statistical Analysis System, SAS Institute Inc., Cary, NC, USA), version 9.4, and statistical significance was defined as p < 0.05.
Of the 8581 participants (49.17% women), the majority self-reported themselves as pardo [4,882, 56.76% (95% CI 54.82–58.70%) and socio-economic class C [4,578, 55.75% (95% CI 53.84–57.67%). The mean age was 21.40 years (21.30–21.51). From the total sample, 8076 provided information about syphilis, and 224 (2.86%, 95% CI 2.29–3.43%) participants reported having been diagnosed with the disease (current or previous). The frequency of syphilis was similar between sexes (p = 0.240), with frequencies of 3.20% (n = 69) for men and 2.54% (n = 155) for women.
Rates of self-reported syphilis were significantly different between socio-economic class: 1.56% class A–B, 2.65% class C, and 4.25% class D–E (p = 0.006), but no differences were found regarding to skin color (p = 0.085) and household income (p = 0.807). The rate of syphilis was higher among smokers (7.11% smoker, 3.06% ex-smoker, and 1.85% nonsmoker, p < 0.001), those who consume drugs (5.09% vs. 1.88% non-drug users, p < 0.001), and alcohol during lifetime (3.36% vs. 1.63, p < 0.001).
In relation to sexual behavior, participants without a partner had higher rate of the disease when compared to participants with a stable partner (3.97% vs. 2.51%, p < 0.026). The same was found with higher number of partners in the past year (5.01% vs. 1.76%, p < 0.001) and/or in those with less current condom use (3.54% vs. 1.89%). Those who had at least one homosexual relationship had a syphilis rate fivefold higher (10.80% vs. 1.98%, p < 0.001). The majority of participants who reported homosexual relationship belonged to social class A–B (11.31%); however, among these participants, the prevalence of syphilis was significantly higher only in social class A–B (10.41% vs. 0.41%, p < 0.001) and C (11.52% vs. 1.52%, p < 0.001), but no significant difference was found in class D (8.89% vs. 3.96%, p = 0.211).
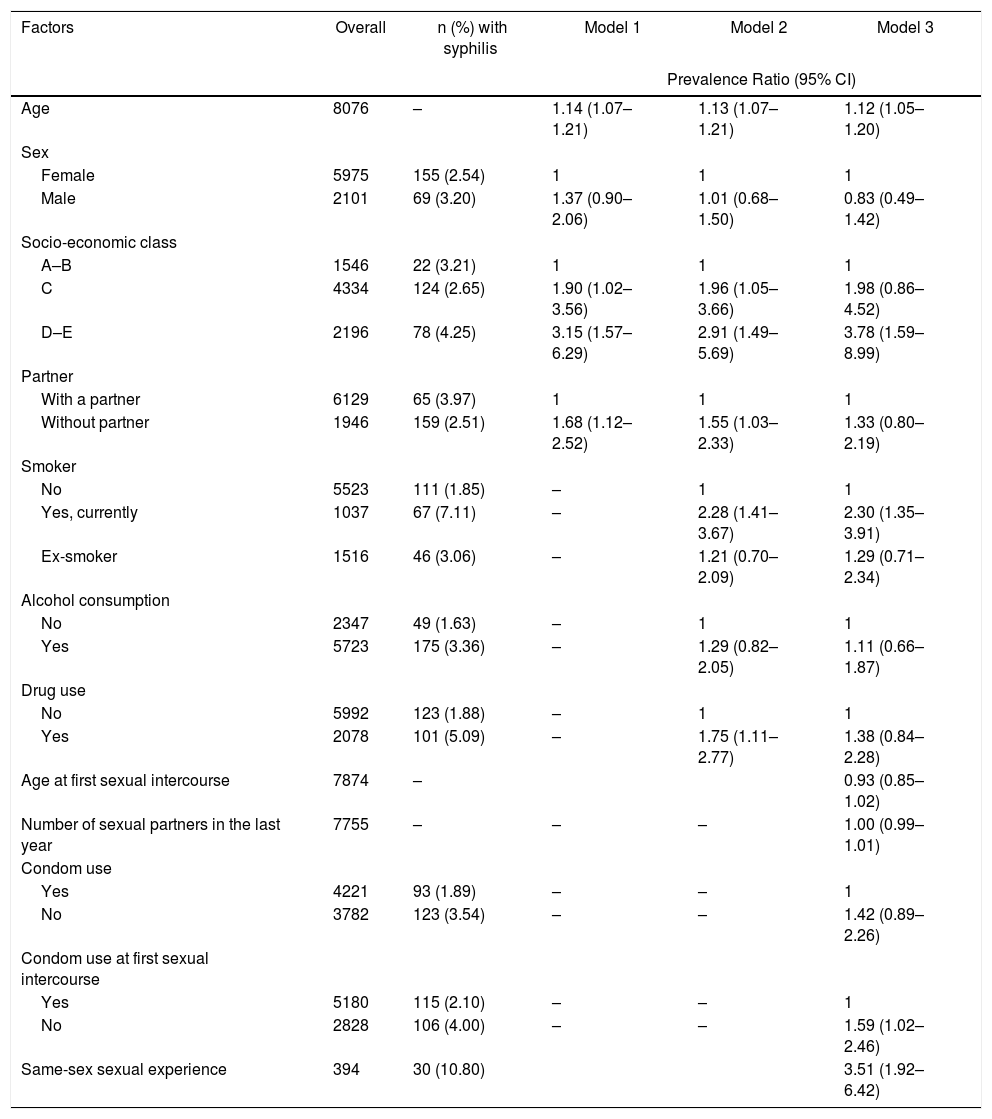
In the multivariate full model, the characteristics associated with self-reported syphilis were age, a lower socio-economic class, smoking, not using a condom at first sexual intercourse, and ever having had a same-sex sexual experience (Table 1). Age and socio-economic class were significant in all models, and the effect size of social class D increased when sexual behaviors were included in the full model. Conversely, social class C and drug was no longer significant. As the lower social class had a higher prevalence of syphilis, and the social class A–B had a higher frequency of same-sex relationship, we tested for interaction between these two variables. However, there was no interaction, meaning that the increase in the prevalence of syphilis in class C was not due to same-sex relationship.
Associated factors for self-reported syphilis among participants aged 16–25 years.
| Factors | Overall | n (%) with syphilis | Model 1 | Model 2 | Model 3 |
|---|---|---|---|---|---|
| Prevalence Ratio (95% CI) | |||||
| Age | 8076 | – | 1.14 (1.07–1.21) | 1.13 (1.07–1.21) | 1.12 (1.05–1.20) |
| Sex | |||||
| Female | 5975 | 155 (2.54) | 1 | 1 | 1 |
| Male | 2101 | 69 (3.20) | 1.37 (0.90–2.06) | 1.01 (0.68–1.50) | 0.83 (0.49–1.42) |
| Socio-economic class | |||||
| A–B | 1546 | 22 (3.21) | 1 | 1 | 1 |
| C | 4334 | 124 (2.65) | 1.90 (1.02–3.56) | 1.96 (1.05–3.66) | 1.98 (0.86–4.52) |
| D–E | 2196 | 78 (4.25) | 3.15 (1.57–6.29) | 2.91 (1.49–5.69) | 3.78 (1.59–8.99) |
| Partner | |||||
| With a partner | 6129 | 65 (3.97) | 1 | 1 | 1 |
| Without partner | 1946 | 159 (2.51) | 1.68 (1.12–2.52) | 1.55 (1.03–2.33) | 1.33 (0.80–2.19) |
| Smoker | |||||
| No | 5523 | 111 (1.85) | – | 1 | 1 |
| Yes, currently | 1037 | 67 (7.11) | – | 2.28 (1.41–3.67) | 2.30 (1.35–3.91) |
| Ex-smoker | 1516 | 46 (3.06) | – | 1.21 (0.70–2.09) | 1.29 (0.71–2.34) |
| Alcohol consumption | |||||
| No | 2347 | 49 (1.63) | – | 1 | 1 |
| Yes | 5723 | 175 (3.36) | – | 1.29 (0.82–2.05) | 1.11 (0.66–1.87) |
| Drug use | |||||
| No | 5992 | 123 (1.88) | – | 1 | 1 |
| Yes | 2078 | 101 (5.09) | – | 1.75 (1.11–2.77) | 1.38 (0.84–2.28) |
| Age at first sexual intercourse | 7874 | – | 0.93 (0.85–1.02) | ||
| Number of sexual partners in the last year | 7755 | – | – | – | 1.00 (0.99–1.01) |
| Condom use | |||||
| Yes | 4221 | 93 (1.89) | – | – | 1 |
| No | 3782 | 123 (3.54) | – | – | 1.42 (0.89–2.26) |
| Condom use at first sexual intercourse | |||||
| Yes | 5180 | 115 (2.10) | – | – | 1 |
| No | 2828 | 106 (4.00) | – | – | 1.59 (1.02–2.46) |
| Same-sex sexual experience | 394 | 30 (10.80) | 3.51 (1.92–6.42) | ||
Model 1: age, sex, socio-economic class, and partner. Model 2: Model 1 + smoking, alcohol consumption, and drug use. Model 3: Model 2 + age at first sexual intercourse, number of sexual partners in the last year, condom use, condom use at first sexual intercourse, and ever having had a same sex experience. p < 0.05.
Skin color and socio-economic class were independently associated with self-reported syphilis (data not shown). However, when both factors were included in the model, skin color lost significance, although no interaction was observed between these variables (p = 0.09).
The infection was associated with a lower socio-economic class, age, current smoking, not using a condom during first sexual intercourse, and ever having had a same-sex sexual experience. Similar frequencies of self-reported syphilis in young adults between sexes were found.
Several important differences exist in coverage, access, surveillance, and provision of primary care, in part due to inequalities in healthcare management and social disparities, with important repercussions on access and use of health services.8 Furthermore, cultural differences exist in sexual behaviors, and the probability of showing risky sexual behaviors may differ by sex similar to other cultural behaviors.8
This was a nationwide study with weighted sample and socio-demographic characteristics of the participants similar to those of the Brazilian population. No other studies were found comparing self-reported syphilis during life in similar populations, but the prevalence was much higher than that of a previous study among conscripts aged 17–20 years that found a syphilis prevalence of 0.53%.9 However, some limitations should be noted. Blood samples were not collected to assess the prevalence of syphilis. Syphilis is often asymptomatic, especially in women, and thus subjects may not have been aware or may have been unwilling to admit that they have had syphilis which may lead to under-reporting of cases. In addition, we must emphasize that the data represent non-probabilistic cases that occurred during the entire lifespan.
Socio-demographic factors, especially socio-economic class, should be considered when planning strategies to prevent and control syphilis, since certain groups are at higher risk in addition to people who exhibit certain sexual behaviors, such as not using a condom at their first sexual intercourse and ever having had a same-sex sexual experience. Several traditional sexual behaviors, such as age of first sexual intercourse and number of sexual partners, were not associated with syphilis. Even so, is desirable that syphilis prevention includes strategies as close language to the youth, training of teachers/educators, easier access to prevention inputs, and condoms distribution in primary care services, focusing in sexual education and condom use from the beginning of sexual activity, especially among lower socio-economic classes.
Conflict of interestThe authors declare that they have no competing interests.
Key points- 1
This is a cross-sectional study with 8,071 participants recruited from 119 primary care units in Brazil.
- 2
The prevalence of self-reported syphilis was 2.86% (95% CI, 2.29–3.43).
- 3
Age, lower socio-economic class, being a smoker, not using a condom at first sexual intercourse, and ever had a same-sex sexual experience were associated with syphilis.
- 4
Syphilis prevention strategies should focus mainly on condom use from the beginning of sexual activity among lower social classes.
