



The ratio of monocytes to lymphocytes in peripheral blood could reflect an individual's immunity to Mycobacterium tuberculosis. The objective of this study was to evaluate the relationship between ratio of monocytes to lymphocytes and clinical status of patients with active tuberculosis.
MethodsThis was a retrospective review of data collected from the clinical database of The Fifth People's Hospital of Wuxi, Medical College of Jiangnan University. A total of 419 patients who had newly diagnosed active tuberculosis and 108 cases from 419 patients with tuberculosis therapy either near completion or completed were selected. Controls were 327 healthy donors.
ResultsMedian ratio of monocytes to lymphocytes was 0.36 (IQR, 0.22–0.54) in patients before treatment, and 0.16 (IQR, 0.12–0.20) in controls (p<0.001). Ratio of monocytes to lymphocytes <9% or >25% was significant predictors for active tuberculosis (OR=114.73, 95% CI, 39.80–330.71; OR=89.81, 95% CI, 53.18–151.68, respectively). After treatment, the median ratio of monocytes to lymphocytes recovered to be nearly normal. Compared to other patients, patients with extrapulmonary tuberculosis and of age >60 years were more likely to have extreme ratio of monocytes to lymphocytes (AOR=2.57, 95% CI, 1.08–6.09; AOR=4.36, 95% CI, 1.43–13.29, respectively).
ConclusionsRatio of monocytes to lymphocytes <9% or >25% is predictive of active tuberculosis.
Globally there were an estimated 8.6 million new cases of tuberculosis (TB) in 2013 and 1.3 million deaths.1 China and India have the greatest burden of disease. India and China alone accounted for 26% and 12% of total cases, respectively.1 In the most Western European countries and United States, the majority of cases occur in foreign-born residents and recent immigrants from countries in which TB is endemic.2–4 TB is presenting new challenges as a global health problem, especially with new threats of HIV coinfection and drug-resistant strains of Mycobacterium tuberculosis (Mtb).5 The knowledge about the hematological manifestations of Mtb infection is critically important to provide insight into pathogenesis. For decades, myeloid-specific cells have been known to serve as host cells for Mtb growth and lymphoid cells are thought to be the major effector cells in TB immunity. Given the central role of monocytes and lymphocytes in the induction of immune responses, their levels (hereafter termed “ML ratio”) in peripheral blood might be expected to reflect the state of an individual's immunity to infection.
In a recent clinical analysis of peripheral blood mononuclear cells from a cohort of South African infants the relative ratio of monocytes to lymphocytes at the start of monitoring was shown to predict risk of developing tuberculosis disease during follow-up.6
Others reported that the ratio of lymphocytes to monocytes in peripheral blood correlated with the extent of tuberculosis in both rabbits7 and humans,8 but the numbers studied were small and the strength of the conclusions that could be reached in humans was deemed to be modest. The direct characterization of ML ratio to date has been surprisingly limited. There was no strong evidence that ML ratio was affected by Mtb infection in humans.
To start with this, using full differential blood count data from patients with active tuberculosis and healthy donors, we sought to determine whether ML ratio could be affected by tuberculosis or ongoing anti-TB treatment and provide insight into its pathogenesis.
MethodStudy population and ethics statementData from all subjects in the present retrospective review were collected from the clinical database of The Fifth People's Hospital of Wuxi, Affiliated to Jiangnan University, between December 2010 and June 2013. This study was approved by the Institutional Ethics Committee of The Fifth People's Hospital of Wuxi, Affiliated to Jiangnan University (QD-2013-0016), and was in compliance with the national legislation and the Declaration of Helsinki guidelines. Written patient consent was obtained according to the institutional guidelines.
Participants clinical diagnosis and treatmentHealthy donors were from the physical examination center of our hospital and met the following criteria: no history of previous active TB or TB treatment, no evidence of current active TB (absence of cough, intermittent fever, and excessive night sweating in the past two weeks and absence of unexplained weight loss in the past month). Tuberculosis was diagnosed when subjects with clinical and/or imaging features compatible with tuberculosis had at least one of the following criteria: positive sputum smear for acid-fast bacilli (AFB); positive culture for M. tuberculosis; biopsy suggestive of tuberculosis, and/or full response to anti-tuberculosis treatment. Patients with extrapulmonary TB accompanying pulmonary TB involvement were included in the category of extrapulmonary TB. Treatment of new cases, both pulmonary and extrapulmonary tuberculosis, received two months of isoniazid (H), rifampicin (R), pyrazinamide (Z) and ethambutol (E) during an intensive phase and four months of HR in the continuation phase. The duration of treatment was six months. Several kinds of extrapulmonary tuberculosis were more difficult to cure. Treatment for an extended period of time was required to ensure disease control. Such as, prolonged therapy had been adopted in TB meningitis (9–12 months) and bone and joint TB (9 months; Fig. 1).9
Full differential blood counts
Full blood counts (FBC) of peripheral blood collected in ethylene-diamine tetra-acetic acid containing (EDTA) tubes were performed by one of two clinical diagnostic laboratories each using a five-part differential hematology analyser (Sysmex Model XS, Hamburg, Germany). Full blood count measurement was subject to strict quality assurance procedures including twice-daily high and low internal quality control, fortnightly quality controls done by the Wuxi clinical laboratory QC scheme (Wuxi, Jiangsu, China) and annual quality assurance as part of Jiangsu clinical laboratory QC scheme. Both laboratories are accredited by the China National Accreditation System in accordance with international standards ISO 17025/2005 and ISO 15189/2007.
Statistical methodsStatistical analysis was conducted using SPSS version 17.0. Pearson's chi-square test and Mann–Whitney U test were used to identify significant differences across patients and healthy donors, patients before treatment and after treatment. p<0.05 (two-sided) was considered as statistically significant difference. The odds ratios (OR) were estimated with 95% confidence intervals (CIs) from the univariate analysis to investigate the relationship between active tuberculosis and the different ML ratios. Adjusted odds ratios (AOR) with 95% CIs were also estimated from the multivariate analysis to determine the factors associated with the different ML ratios of patients.
ResultsCharacteristics of the study populationA total of 1068 patients were diagnosed with active TB in the database of The Fifth People's Hospital of Wuxi from December 2010 to June 2013. Availability of full differential blood counts when newly diagnosed with active TB (previously untreated for TB and never received anti-TB drugs for <1 month) was required to compare with healthy donors. Patients without pre-treatment data were excluded and 965 patients remained. We further excluded return-visiting patients, who experienced treatment failure or reinfection during the course of therapy, 638 patients remained. After excluding patients with viral hepatitis (viral hepatitis type A, B and C), AIDS (acquired immune deficiency syndrome), and diabetes, 464 patients remained. Individuals who were pregnant, did not agree to participate in our study, or had other diseases, such as, lung cancer, measles, syphilis, leucopenia, systemic lupus erythematosus, or rheumatoid arthritis, which were likely to influence full blood counts, were also excluded. Finally, data of full blood counts from 419 patients were included in the analysis, with a median age of 55 years, and 71.1% were men. Furthermore, in order to assess the influence of anti-TB therapy, we excluded patients who did not receive the recommended therapy, such as irregular treatment, intermittent treatment, and undertreated patients. Finally, 108 patients who had anti-TB therapy either near completion or completed remained. A total of 327 healthy volunteers were included, 207 male and 120 female subjects.
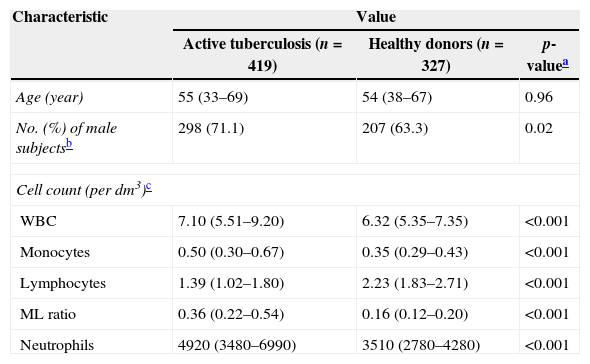
Demographic, clinical, and laboratory characteristics of the study sampleThere were 746 individuals enrolled in the study: 419 patients with newly treated active tuberculosis, and 327 healthy donors without Mtb infection. Demographic and clinical characteristics and laboratory data are summarized in Table 1. There was no difference in median age or sex between patients and healthy donors. Patients with active tuberculosis had significantly higher median absolute number of white blood cell (WBC), monocytes and neutrophils than healthy donors. The median absolute number of lymphocytes of patients was significantly lower than that of healthy donors. Patients with active tuberculosis had a significantly different ML ratio to healthy donors.
Demographic, clinical, and laboratory characteristics of the study population.
| Characteristic | Value | ||
|---|---|---|---|
| Active tuberculosis (n=419) | Healthy donors (n=327) | p-valuea | |
| Age (year) | 55 (33–69) | 54 (38–67) | 0.96 |
| No. (%) of male subjectsb | 298 (71.1) | 207 (63.3) | 0.02 |
| Cell count (per dm3)c | |||
| WBC | 7.10 (5.51–9.20) | 6.32 (5.35–7.35) | <0.001 |
| Monocytes | 0.50 (0.30–0.67) | 0.35 (0.29–0.43) | <0.001 |
| Lymphocytes | 1.39 (1.02–1.80) | 2.23 (1.83–2.71) | <0.001 |
| ML ratio | 0.36 (0.22–0.54) | 0.16 (0.12–0.20) | <0.001 |
| Neutrophils | 4920 (3480–6990) | 3510 (2780–4280) | <0.001 |
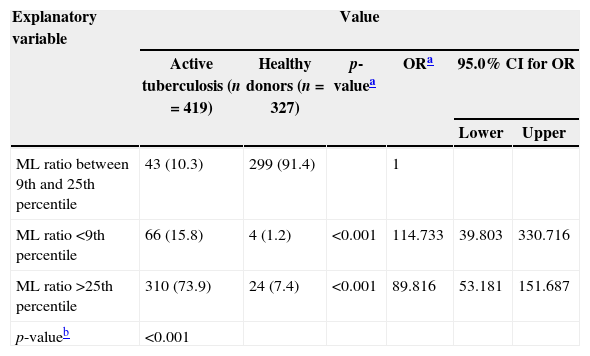
Participants (patients and healthy donors) were stratified into categories of ML ratio of less than the 9th percentile, between the 9th and 25th percentile, and greater than the 25th percentile (Table 2). Compared to healthy donors, patients with active tuberculosis were distributed differently in the three categories: 73.9% of patients compared to 24% of healthy donors with ML ratio >the 25th percentile, 15.8% to 1.2% with ML ratiop<0.001) (Table 2). As shown in Fig. 2, ML ratio of healthy donors (blue circle) centralized mostly between the blue and green lines (91.4%); ML ratio of patients (green circle) distributed mainly out of the lines (89.7%) (Fig. 2A). ML ratio of healthy donors was the most centralized data (IQR 0.08), and gathered mainly in the area where the data from patients distributed rarely (Fig. 2B). Compared to ML ratio between the 9th and 25th percentile, participants with ML ratio
Percentile ranking of the ratio of monocytes to lymphocytes.
| Explanatory variable | Value | |||||
|---|---|---|---|---|---|---|
| Active tuberculosis (n=419) | Healthy donors (n=327) | p-valuea | ORa | 95.0% CI for OR | ||
| Lower | Upper | |||||
| ML ratio between 9th and 25th percentile | 43 (10.3) | 299 (91.4) | 1 | |||
| ML ratio <9th percentile | 66 (15.8) | 4 (1.2) | <0.001 | 114.733 | 39.803 | 330.716 |
| ML ratio >25th percentile | 310 (73.9) | 24 (7.4) | <0.001 | 89.816 | 53.181 | 151.687 |
| p-valueb | <0.001 | |||||
 with ratio of monocytes to lymphocytes (ML ratio). (A) Monocytes and lymphocytes count are plotted on the x- and y-axes, respectively. ML ratio of healthy donors (blue circle) centralized mostly between the blue and green lines, ML ratio of patients (green circle) distributed mainly out of the lines. The dotted blue line denotes the 9th percentiles for ML ratio. The dotted green line denotes the 25th percentiles for ML ratios. (B) Median levels of ML ratio of patients of active tuberculosis and healthy donors. Each dot represents ML ratio for an individual patient or healthy donor. Bars represent medians. ML ratio of healthy donors gathered mainly in the area where the data from patients distributed rarely.")
Distribution of participants (patients and healthy donors) with ratio of monocytes to lymphocytes (ML ratio). (A) Monocytes and lymphocytes count are plotted on the x- and y-axes, respectively. ML ratio of healthy donors (blue circle) centralized mostly between the blue and green lines, ML ratio of patients (green circle) distributed mainly out of the lines. The dotted blue line denotes the 9th percentiles for ML ratio. The dotted green line denotes the 25th percentiles for ML ratios. (B) Median levels of ML ratio of patients of active tuberculosis and healthy donors. Each dot represents ML ratio for an individual patient or healthy donor. Bars represent medians. ML ratio of healthy donors gathered mainly in the area where the data from patients distributed rarely.
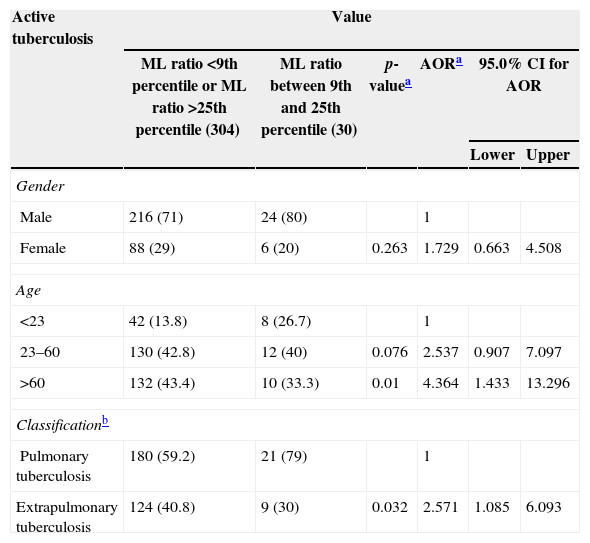
A multivariate analysis was conducted using variables of gender, age and disease classification. As shown in Table 3, our study compared the characteristics of 334 from 419 patients who had clear information of disease classification. Male patients had a higher probability to be in the group of ML ratio <9% or ML ratio >25% than female patients, but the result had no statistical significance. Compared to patients less than 23 years of age, patients older than 60 years were over 4-fold more likely to be in the group of ML ratio <9% or ML ratio >25%. Patients with extrapulmonary tuberculosis were nearly 2.5-fold more likely to be in the extreme groups (Table 3).
Factors associated with different ML ratios distribution of patients diagnosed with active tuberculosis.
| Active tuberculosis | Value | |||||
|---|---|---|---|---|---|---|
| ML ratio <9th percentile or ML ratio >25th percentile (304) | ML ratio between 9th and 25th percentile (30) | p-valuea | AORa | 95.0% CI for AOR | ||
| Lower | Upper | |||||
| Gender | ||||||
| Male | 216 (71) | 24 (80) | 1 | |||
| Female | 88 (29) | 6 (20) | 0.263 | 1.729 | 0.663 | 4.508 |
| Age | ||||||
| <23 | 42 (13.8) | 8 (26.7) | 1 | |||
| 23–60 | 130 (42.8) | 12 (40) | 0.076 | 2.537 | 0.907 | 7.097 |
| >60 | 132 (43.4) | 10 (33.3) | 0.01 | 4.364 | 1.433 | 13.296 |
| Classificationb | ||||||
| Pulmonary tuberculosis | 180 (59.2) | 21 (79) | 1 | |||
| Extrapulmonary tuberculosis | 124 (40.8) | 9 (30) | 0.032 | 2.571 | 1.085 | 6.093 |
In order to further evaluate the impact of anti-TB therapy on the ML ratio, we excluded patients who did not receive the recommended therapy, such as irregular treatment, intermittent treatment, and undertreated therapy. A total of 108 from 419 patients who had FBC with therapy either near completion or completed were remaining and was also stratified into the same three categories with ML ratio: less than the 9th percentile, between the 9th and 25th percentile, and greater than the 25th percentile. Anti-TB therapy significantly reduced ML ratio with ML ratio greater than 25th percentile (median ML ratio, 0.472 (IQR, 0.33–0.62) before treatment vs 0.2199 (IQR, 0.16–0.28) after treatment, p<0.001). ML ratio elevated significantly with ML ratio less than 9th percentile (median ML ratio, 0.026 (IQR, 0.006–0.059) before treatment vs 0.197 (IQR, 0.09–0.25) after treatment, p<0.001). In patients with ML ratio between the 9th and 25th percentile, there was no difference between ML ratio before treatment (median ML ratio, 0.20 [IQR 0.15–0.23]) and after treatment (median ML ratio, 0.15 [IQR, 0.12–0.19], p=0.166). Before anti-TB therapy, 9.3% of individuals (10/108) had ML ratio between the 9th and 25th percentile, compared with 75% (81/108) following anti-TB therapy (p<0.001). The median ML ratio of healthy donors was 0.15 (IQR, 0.12–0.19). The results indicated that higher ML ratio decreased, and lower ML ratio increased to be close to the ML ratio of healthy donors. ML ratio of patients recovered to be nearly normal with treatment.
DiscussionMonocytes are an essential component of the innate immune response that acts as a link to the adaptive immune system through antigen presentation to lymphocytes. Thus any factor that perturbs the function or relative numbers of either cell type could potentially affect an individual's response to infection.
The ML ratio in peripheral circulation may reflect an individual's capacity to mount an effective immune response. ML ratio has been shown to correlate with inhibition of mycobacterial growth in vitro10,11 and the risk is higher among individuals with either low or high ML ratio.12 These results add to evidence supporting that extremes of immunity are associated with TB. This ratio could herald a previously unknown pathophysiologic change of TB. As demonstrated by our study, patients with active tuberculosis had a higher or lower ML ratio compared to healthy donors. We stratified participants into three categories with different ML ratios, and healthy donors were mostly in the group of ML ratio between the 9th and 25th percentile, but patients were mainly in the group of ML ratio greater than the 25th percentile and in the group of ML ratio less than the 9th percentile (Table 2). ML ratios in extreme percentiles were significant predictors for active tuberculosis.
The normal ML ratio is disrupted by Mtb infection. It has been reported recently that Mtb infection may alter subsets of hematopoietic stem cells13 or directly infect bone marrow mesenchymal stem cells.14 Studies in mice15 and humans16 have shown that subsets of hematopoietic stem cells have distinct biases in the ratio of myeloid to lymphoid cells they give rise to.17,18 The different proportion of myeloid biased or lymphoid-biased hematopoietic stem cells may underlie the peripheral difference of ML ratio. Therefore, it is reasonable that Mtb infection may alter hematopoietic stem cells such that the ML ratio is altered. The change of monocytes and lymphocytes, reflected in their ratio, may affect patients’ ability to respond to mycobacterial infection. Further work to explore the pathophysiological involvement of the ML ratio in TB may yield new pathways to modify or prevent the disease.
ML ratio of patients aged more than 60 years and extrapulmonary tuberculosis are disrupted more seriously than others. The multivariate analysis indicated that, among patients diagnosed with active tuberculosis, to be aged more than 60 years and to have extrapulmonary tuberculosis were associated with different ML ratios of patients.
In order to further evaluate whether ML ratio could be affected by anti-TB therapy, the difference between before treatment and after therapy was analyzed (Fig. 3). The results indicated that high ML ratio decreased, and low ML ratio increased to be close to the ML ratio of healthy donors. It suggested that ML ratio of patients may be changed with anti-TB therapy and the alteration of ML ratio may also reflect the effectiveness and phase of therapy.
 of patients, before treatment, after treatment and healthy donors. (A) ML ratio of patients with ML ratio greater than 25th percentile; (B) ML ratio of patients with ML ratio less than the 9th percentile; (C) ML ratio of patients with ML ratio between the 9th and 25th percentile. Data are presented with box plot reporting the median values and the interquartile range (***p<0.001). Median ML ratio of patients changed to be close to healthy donors with anti-tuberculosis treatment.")
Ratio of monocytes to lymphocytes (ML ratio) of patients, before treatment, after treatment and healthy donors. (A) ML ratio of patients with ML ratio greater than 25th percentile; (B) ML ratio of patients with ML ratio less than the 9th percentile; (C) ML ratio of patients with ML ratio between the 9th and 25th percentile. Data are presented with box plot reporting the median values and the interquartile range (***p<0.001). Median ML ratio of patients changed to be close to healthy donors with anti-tuberculosis treatment.
Our study has several limitations. The eligible patients represented a fraction of the patients diagnosed with active tuberculosis during the study period, raising a concern for a selection bias. Nearly 60.8% (649/1068) of the patients were excluded. Whether the exclusion of these patients affected the outcome is unknown. As a retrospective study, collecting information from medical records filled in by other professionals is unavoidable but tends to be less accurate. Fortunately, at the time of clinical assessment, although clinicians were not blinded to the full blood count, they were not aware of this hypothesis, thus diminishing diagnostic bias.
Despite these limitations, our results support that ML ratios are disrupted with tuberculosis; ML ratios in the extreme percentiles are associated with active TB. This observation needs to be confirmed in other geographic settings.
Conflicts of interestThe authors declare no conflicts of interest.
We thank the all patients for their support in this research and colleagues of The Fifth People's Hospital of Wuxi for their assistance in collection of research data.
