
Norovirus (NoV) and Rotavirus (RoV) are the major cause of outbreaks and sporadic gastroenteritis worldwide. NoV has become the leading cause of acute gastroenteritis (AGE) in all age groups.1 The aim of the study was to identify NoV infection, to know the clinical characteristics and its association with RoV infection in children aged less than five years hospitalized at the Havana Centre Paediatric Hospital, Havana, Cuba, due to AGE, from March 2010 to February 2011.
Eighty-eight stool samples collected from children aged less than five years were studied. RoV and NoV antigens were detected by ELISA (IDEIA™ Rotavirus, OXOID Ltd., United Kingdom) and RT-PCR respectively.2 The SPSS programme (SPSS Inc., Chicago, IL) was used for the statistical analysis.
Fifty-four samples (61.4%) turned out positive for RoV and 31.8% (28/88) were positive for NoV (p>0.05). Infections of RoV were seen in 51.9% of male children (28/54), whereas NoV infections were observed in 53.6% (15/28) of female patients (p>0.05).
Among positive patients, NoV genogroup GII was the most prevalent, detected in 78.6% (22/28). Mixed infections were identified in 20.5% patients (18/88).
The peak incidence of infection (RoV/81.5%; NoV/82.1%) was in children under 12 months. No death was reported.
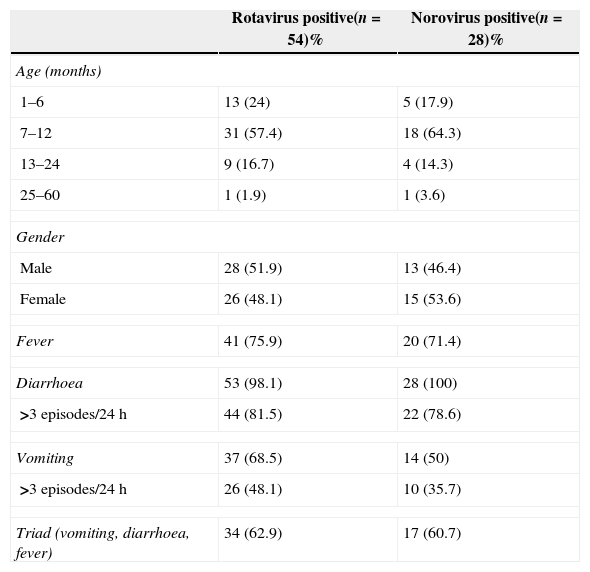
The clinical features of patients with RoV and NoV infections are displayed in Table 1. RoV positive cases had more episodes of diarrhoea in 24h (81.5%) than cases of NoV infection (78.6%).
Clinical characteristics of Norovirus and Rotavirus infection, in children under 5 years old.
| Rotavirus positive(n=54)% | Norovirus positive(n=28)% | |
|---|---|---|
| Age (months) | ||
| 1–6 | 13 (24) | 5 (17.9) |
| 7–12 | 31 (57.4) | 18 (64.3) |
| 13–24 | 9 (16.7) | 4 (14.3) |
| 25–60 | 1 (1.9) | 1 (3.6) |
| Gender | ||
| Male | 28 (51.9) | 13 (46.4) |
| Female | 26 (48.1) | 15 (53.6) |
| Fever | 41 (75.9) | 20 (71.4) |
| Diarrhoea | 53 (98.1) | 28 (100) |
| >3 episodes/24h | 44 (81.5) | 22 (78.6) |
| Vomiting | 37 (68.5) | 14 (50) |
| >3 episodes/24h | 26 (48.1) | 10 (35.7) |
| Triad (vomiting, diarrhoea, fever) | 34 (62.9) | 17 (60.7) |
Clinical sings and symptoms were not different between RoV and NoV case-patients. However, fever (41/75.9%) and vomiting (37/68.5%) were more common in RoV compared to NoV infection (fever – 20/71.4%; vomiting – 14/50%) (p>0.05). The classic triad of symptoms (diarrhoea, vomiting, and fever) occurred in 62.9% of RoV and 46.4% of NoV infected children.
RoV and NoV were detected year round; however, the infection peaked in the months from December to February: 62.9% (34/54) and 60.7% (17/28) of RoV and NoV respectively.
In conclusion, it was found that RoV continues to be a common etiological agent of diarrhoea in hospitalized children aged less than five years, as has been reported previously.3,4 However, the laboratory limitations to detect sporadic cases of NoV in paediatric hospitals, underestimate diagnosis of this infection.
Of the NoV genogroups, GII was predominant, which was consistent with studies conducted in other settings.5
A seasonal pattern of RoV and NoV was not noted, because samples were not collected every month. Clear seasonality in RoV infection in the country has not been demonstrated, although a high frequency has been found during winter months.1,3
In the study, RoV and NoV clinical characteristics were mostly indistinguishable, although some authors consider vomiting associated to NoV infection more frequently.1,5
Mixed infection among RoV and NoV was observed in children aged less than one year. Different factors can cause infection in these children, as early breastfeed replacement and the hygienic measures taken by adults who work with children.5
This study confirms the importance of NoV and RoV infection in hospitalized children aged less than five years. Further studies integrating other virus in the diagnosis of AGE need to be undertaken.
Conflicts of interestThe authors declare no conflicts of interest.
