



Systemic microvascular dysfunction has been shown to be present in COVID-19, and serum cytokines are known to be involved in the regulation of vascular function. We sought to evaluate systemic microvascular endothelial function, with laser doppler perfusion monitoring (LDPM), and plasma levels of cytokines after acute COVID-19. Individuals admitted to a Cardiology hospital with acute COVID-19 and followed for 12–15 months after recovery underwent noninvasive evaluation of systemic endothelium-dependent microvascular reactivity by cutaneous LDPM with local thermal hyperemia (LTH). A multiplex biometric immunoassay panel was used to assess 48 serum cytokines and chemokines. Twenty patients and 14 control volunteers were enrolled. The areas under the curves of vasodilation induced by LTH were significantly increased after recovery (P=0.009) and were not different from values obtained in healthy volunteers (P = 0.85). The peak microvascular flow during LTH did also significantly increase (P = 0.02), and was not different form values obtained in healthy volunteers (P = 0.55). Several cytokines displayed significantly reduced serum concentrations after recovery from COVID-19. In conclusion, endothelium-dependent systemic microvascular reactivity improved after recovery from COVID-19 in patients with cardiovascular diseases, in parallel with a reduction in the levels of several serum cytokines and chemokines involved in the regulation of vascular function and inflammation.
Systemic microvascular dysfunction has been shown to play a crucial role in the pathophysiology of coronavirus disease 2019 (COVID-19).1–3 Persistent endothelial dysfunction, assessed through changes in endothelium-dependent flow-mediated dilation, has been detected in post-acute COVID-19 patients, two months after a SARS-CoV-2 negative nasopharyngeal swab,4 with significant improvement after multidisciplinary rehabilitation.5 Moreover, the improvement in endothelial function was positively correlated with the improvement in pulmonary function.4
We have recently shown that patients with acute COVID-19 and cardiovascular disease developed systemic microvascular endothelial dysfunction, in parallel with marked increases in the levels of serum cytokines and chemokines involved in the regulation of vascular function and inflammation.6 In addition, also using cutaneous laser Doppler flowmetry, Glazkov et al.7 reported that known COVID-19 risk factors, including hemorheological parameters and age, are negatively correlated with endothelium-dependent microvascular reactivity to heating in patients with COVID-19. Moreover, patients with COVID-19, particularly those with severe infection, have a reduced hyperemic coronary flow and coronary flow velocity reserve, indicating the presence of coronary microvascular dysfunction, which correlates with biomarkers of inflammation.8
However, the evolutionary pattern of systemic microcirculatory function after recovery remained to be investigated. Therefore, we sought to evaluate whether systemic microvascular endothelial dysfunction, assessed with lased doppler perfusion monitoring (LDPM), and increased plasma levels of cytokines and chemokines persisted 12 to 15 months after acute COVID-19.
Twenty patients who had been admitted with COVID-19 to the National Institute of Cardiology, in Rio de Janeiro, Brazil, during 2020 were studied 12 to 15 months after the acute phase of the disease. All patients had underlying cardiac disease and signed an informed consent to participate. The study was approved by the Institutional Review Board (protocol number CAAE 31237220.1.0000.5272) and was registered and made public at ClinicalTrials.gov (NCT4406545).
The patients had SARS-CoV-2 infection detected by RT–PCR analysis of nasopharyngeal swabs and met the criteria for hospitalization either due to their underlying condition or due to COVID-19 severity.9 During the follow-up evaluation for this study, all patients had negative RT–PCR tests for COVID-19. Serum cytokines were evaluated on the same day the LDPM was performed.
A group of healthy volunteers (n = 14) without acute or chronic diseases or cardiac risk factors, was recruited among hospital staff members who tested negative for SARS-CoV-2. This group was also evaluated with LDPM and served as a control group, as previously described.6
The evaluation of the microvascular flow and reactivity was performed using a single-point laser Doppler perfusion monitoring (LDPM) system (Periflux 5001, Perimed, Järfälla, Sweden) and heating laser probes (PF 457, Perimed, Järfälla, Sweden) to noninvasively measure systemic microvascular perfusion changes (in arbitrary perfusion units [APU=10 mV]). After measuring the resting microvascular flow on the skin of the forearm for five minutes, endothelium-dependent microvascular vasodilatation was assessed using 15 min local heating of the laser probe to 44°C (local thermal hyperemia, LTH), as previously described.10,11 The areas under the curves (AUCs) of vasodilation induced by LTH and peak microvascular flow during LTH were calculated using Perimed's dedicated software for Perimed Periflux System 5001 (Perimed, Järfälla, Sweden).
Blood samples were collected from a peripheral vein and stored on ice. Plasma was obtained by centrifugation at 800g for 15 min at 4°C, and aliquots were stored at -70°C until the day of analysis. A multiplex biometric immunoassay using fluorescently dyed microspheres conjugated to monoclonal antibodies specific for a target protein was used to measure 48 cytokines and chemokines according to the manufacturer's instructions (Bio-Plex Human Cytokine Assay; Bio-Rad Inc., Hercules, CA, USA). Cytokines and chemokines [IL-1α, IL-15, IL-17, IL-5, IL-10, IFN-α2, IL-12p40, MCP-1, cutaneous T cell-attracting chemokine (CCL247CTACK), IFN-γ-inducible protein-10 (CXCL10/IP-10), monocyte chemoattractant protein-1 (CCL2/MCP-1), macrophage inflammatory protein (CCL3/MIP-1α and CCL4/MIP-1β), and regulated upon activation of normal T cell expression and secretion (CCL5/RANTES)] were determined using a multiplex array reader from the Luminex™ Instrumentation System (Bio-Plex Workstation from Bio-Rad Laboratories, Hercules, California, USA). The analyte concentrations were calculated using software provided by the manufacturer (Bio-Plex Manager Software).
Results are presented as mean ± SD or median (25th–75th percentiles) for the parametric or nonparametric parameters, respectively, according to the Shapiro–Wilk normality test. The statistical analysis of cytokine values was performed using two-tailed paired t tests (parametric values) or Wilcoxon matched-pairs signed rank test (nonparametric values). The microvascular parameters were analyzed using one-way ANOVA (Tukey's multiple comparisons test). The outlier values of microvascular parameters or plasma concentrations of cytokines and chemokines were detected using the robust regression and outlier removal method (ROUT).12P-values < 0.05 were considered statistically significant. All statistical analyses were performed using Prism, version 7.0 (GraphPad Software Inc. La Jolla, CA, USA).
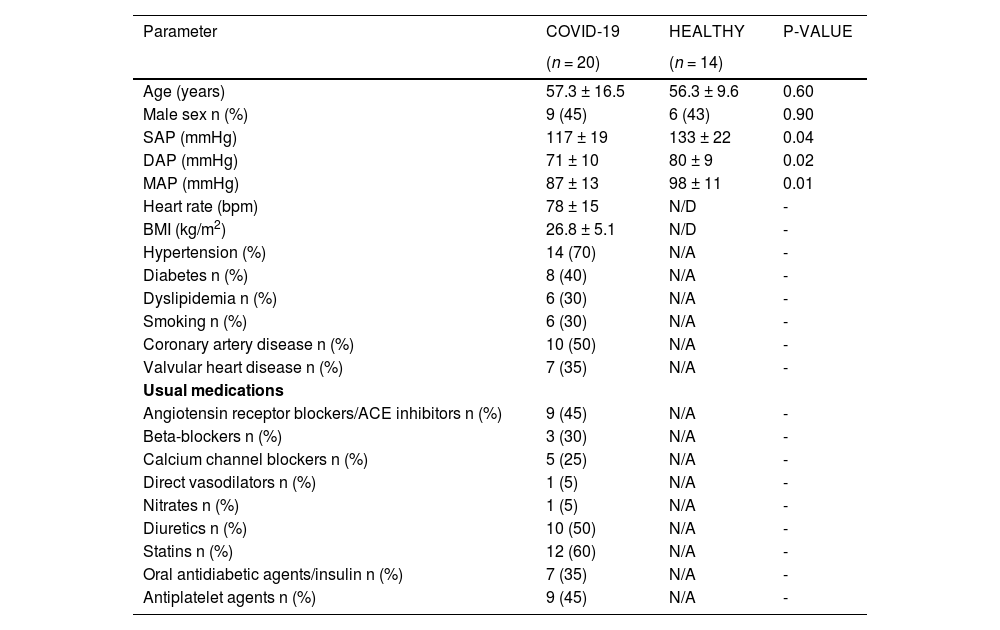
Twenty patients who had mild to moderate COVID-19 were included in the study. The outlier values of microvascular parameters of two patients were excluded from the analysis based on the ROUT. Mean age of the patients and controls was 57.3 ± 16.5 vs 56.3 ± 9.6 years (P = 0.60), and 45% vs. 43% (P = 0.90) were male. Regarding patients, 70% had hypertension, 40% had diabetes, 30% had dyslipidemia, 30% were smokers, 50% had coronary artery disease, and 35% had valvular heart disease; 45% were on angiotensin receptor blockers or angiotensin-converting enzyme inhibitors, 70% on beta-blockers, 25% on calcium channel blockers, 5% on direct vasodilators, 5% on nitrates, 50% on diuretics, 60% on statins, 45% on antiplatelet agents, and 35% on oral antidiabetic agents or insulin. At the follow-up visit, 65% of the patients were symptomatic, with fatigue, dyspnea, cough, headache, anosmia, muscle pain, cognitive and sleep disturbances as the most frequent symptoms; 46% of the patients had more than one symptom.
The evaluation of endothelium-dependent microvascular reactivity showed that vasodilation induced by LTH was significantly increased after recovery compared with values obtained during the acute phase of COVID-19, and similar to that of healthy controls (Fig. 1A). Accordingly, the AUCs of vasodilation were significantly increased after recovery [95,415 (75,552-121,399) vs. 57,555 (40,509-78,310) APU/mmHg/s, P = 0.009] but not different from values obtained in healthy volunteers [111,745 (78,112-123,754) APU/mmHg/s, P = 0.85; Fig. 2B]. The peak microvascular flow during LTH was also significantly increased [116.5 (96.5-144.5) vs. 84 (61.2-140.5) APU, P = 0.02], but not different from values obtained in healthy volunteers [145.5 (119-173.3) APU, P = 0.55; Fig. 2C]. The baseline values of microvascular flow were not different between the recovery period and acute phase [12.5 (8.7-16) vs. 9.5 (7-12.7) APU, P = 0.52] or when compared with those of healthy volunteers [8.5 (6.7-10.5); P = 0.08]. Finally, the comparison of the endothelium-dependent microvascular reactivity in patients with or without symptoms after recovery from COVID-19 showed that vasodilation induced by LTH was not different between these groups (Fig. 3).
 on cutaneous microvascular flow and reactivity in patients during the acute phase of COVID-19 (ACUTE), 12–15 months after recovery (POST-COVID) and in healthy volunteers (HEALTHY): (A) time-course of microvascular vasodilation; (B) areas under the curves of microvascular vasodilation and (C) peak microvascular flow during LTH. The values are expressed as the mean ± SD or median values (25th to 75th percentiles) according to Shapiro–Wilk normality tests. The results were analyzed using one-way ANOVA (Tukey")
Effects of local thermal hyperemia (LTH) on cutaneous microvascular flow and reactivity in patients during the acute phase of COVID-19 (ACUTE), 12–15 months after recovery (POST-COVID) and in healthy volunteers (HEALTHY): (A) time-course of microvascular vasodilation; (B) areas under the curves of microvascular vasodilation and (C) peak microvascular flow during LTH. The values are expressed as the mean ± SD or median values (25th to 75th percentiles) according to Shapiro–Wilk normality tests. The results were analyzed using one-way ANOVA (Tukey's multiple comparisons test). APU, arbitrary perfusion units.
, proinflammatory chemokines (B) and anti-inflammatory cytokines (C) obtained in patients during the acute phase of COVID-19 (ACUTE-COVID) and 12-15 months after recovery (POST-COVID). The results are presented as the mean ± SD or the median (25th–75th percentile) for values that follow or do not follow a Gaussian distribution, respectively (Shapiro–Wilk normality test). P values were estimated using two-tailed paired Student")
Plasma concentrations of proinflammatory cytokines (A), proinflammatory chemokines (B) and anti-inflammatory cytokines (C) obtained in patients during the acute phase of COVID-19 (ACUTE-COVID) and 12-15 months after recovery (POST-COVID).
The results are presented as the mean ± SD or the median (25th–75th percentile) for values that follow or do not follow a Gaussian distribution, respectively (Shapiro–Wilk normality test). P values were estimated using two-tailed paired Student's t tests (parameters with Gaussian distribution) or Wilcoxon matched-pairs signed rank test (parameters with non-Gaussian distribution).
 on cutaneous microvascular flow and reactivity in patients with or without persistent symptoms 12–15 months after infection recovery. The values are expressed as the mean ± SD according to Shapiro-Wilk normality tests. The results were analyzed using two-way ANOVA followed by the Sidak")
Effects of local thermal hyperemia (LTH) on cutaneous microvascular flow and reactivity in patients with or without persistent symptoms 12–15 months after infection recovery. The values are expressed as the mean ± SD according to Shapiro-Wilk normality tests. The results were analyzed using two-way ANOVA followed by the Sidak's multiple comparisons test. There were no significant differences between groups.
APU, arbitrary perfusion units.
Plasma levels of high-sensitivity C-reactive protein in the patients decreased from 3.55 (1.4-10.3) mg/L (acute phase of COVID-19 infection) to 0.2 (0.2–0.4) mg/L after recovery (P = 0.0001). Also, after recovery, patients had significantly lower serum concentrations of the proinflammatory cytokines and chemokines IL-1α, IL-15, IL-17, IFNα2, IL-2p40, MCP-1, MIP1β, RANTES, and CTACK, as well as of the anti-inflammatory cytokines IL-5 and IL-10. However, IP-10 levels increased after recovery (Fig. 2).
Cytokines are well-recognized important parameters in the evaluation of COVID-19, either in the acute phase or in the assessment of disease progression; thus, understanding the qualitative, quantitative, and temporal evolution of cytokine expression is essential for a better comprehension of the disease. Interestingly, in this study, IP-10 serum levels were higher in the follow-up evaluation than during the acute phase of COVID-19. Busko et al.13 reported that IP-10 expression is different in COVID-19 compared to other viral infections, where it is transiently induced, while in the former it has frequently remained elevated. Elevated IP-10 might be a signature of severe coronavirus infection, as it has also been found in SARS-CoV and MERS-CoV infections.
Concerning the dispersion of cytokines levels measured in the present study, it is important to note that factors such as age, sex, and preexisting diseases influence the immune system of patients, reflecting the variable cytokine response to infections. The variability in the pattern of pro-inflammatory cytokines observed in our study is justified because the standard deviation increases as the dispersion around the arithmetic mean increases. The number of patients enrolled for the analysis also contributed for a large dispersion of the results. However, we applied appropriate statistical tests that proved the statistical significance of the results presented.14,15
The interplay between endothelial function and inflammation (expressed by serum cytokines) seems to be key in the pathophysiology of COVID-19, either in the acute phase or after recovery. The inflammatory response driven by several cytokines, including those originating from perivascular adipocytes, may aggravate endothelial dysfunction via endothelial nitric oxide synthase uncoupling and reactive oxygen species production.16
Persistent endothelial dysfunction has been shown after recovery from COVID-19 in some studies.17 Chioh et al.18 found elevated levels of circulating endothelial cells, a biomarker of vascular injury, in patients who recovered from COVID-19, especially in those with preexisting conditions such as hypertension or diabetes. In their study, proinflammatory cytokines (IL-1β, IL-17A, IL-2, and RANTES) remained elevated during early recovery, again more intensely in patients with cardiovascular risk factors, correlating positively with circulating endothelial cell measures, suggesting cytokine-induced endothelial dysfunction (Table 1).
The clinical characteristics of COVID-19 patients and healthy controls evaluated 12-15 months after infection recovery.
SAP, systolic arterial pressure; DAP, diastolic arterial pressure; MAP, mean arterial pressure; ACE, angiotensin-converting enzyme; BMI, body mass index; N/D, not determined; N/A, not applicable.
The results are presented as mean ± SD or median (25th–75th percentile) for values that follow or do not follow a Gaussian distribution, respectively (Shapiro-Wilk normality test).
P-values were estimated using two-tailed unpaired Student's t tests (comparisons of two groups for parameters with Gaussian distribution), two-tailed unpaired Mann-Whitney tests (comparisons of two groups for parameters with non-Gaussian distribution), or chi-square (Fisher's exact test), for categorical parameters.
Long COVID-19, or the presence of symptoms or health disturbances after four weeks from SARS-CoV-2 infection,19 has been a recent matter of concern. In our study, at the follow-up visit, 65% of the patients were symptomatic, but endothelial dysfunction was not associated with either the presence or absence of symptoms. In the study by Charffedine et al.20 77.4% of the patients reported long-COVID symptoms, but endothelial dysfunction, as well as female sex and severity of acute COVID-19, were significantly associated with long COVID-19. Different techniques for the assessment of endothelial function, as well as the small number of patients in our study, may account for the discrepant findings. In our study sample of patients with known cardiovascular disease, both endothelial dysfunction and serum proinflammatory cytokine levels had recovered by the long-term follow-up evaluation, suggesting that it might take much longer to return to baseline states after COVID-19.
While clinical studies on microcirculatory physiology, using different methods,21 have been performed for a long time in the context of several medical conditions, including cardiovascular and metabolic diseases,22 the applications in the study of infectious diseases have been scarce. Nonetheless, using laser-based methodology, we demonstrated that the microcirculation of patients with infective endocarditis have greater basal vasodilation and a reduction of the endothelium-dependent and -independent microvascular reactivity, compared to healthy individuals.23 LDPM is a noninvasive method for the evaluation of systemic microvascular endothelial function,24 as the cutaneous microcirculation is an accessible and representative vascular bed that can be used for the evaluation of systemic microcirculatory flow and reactivity.25 Systemic microvascular reactivity can be evaluated using LDPM combined with cutaneous LTH, as the vasodilatory response in the skin due to LTH represents, fundamentally, endothelium-dependent microvascular reactivity.11,26 Therefore, noninvasive assessment of endothelial function in COVID-19 may help understand the pathophysiology and evolution of the disease.7
Study limitations and strengthsThis was a small study of a specific group of patients with prior cardiac disease; therefore, the results may not be generalizable to other populations with COVID-19 infection. Nonetheless, it may serve as a proof of concept of the reversibility of the acute abnormalities of endothelial function one year after acute COVID-19. Additionally, it depicts the usefulness of a noninvasive method for the evaluation of endothelial function, which may be useful for larger trials.
Funding sourcesThis investigation was supported by grants from CNPq (Conselho Nacional de Desenvolvimento Científico e Tecnológico, E.T. grant #305234/2017-0 and H.C.C.F.N. grant #4017000/2020-8), FAPERJ (Fundação de Amparo à Pesquisa do Estado do Rio de Janeiro, E.T. grant #E-26/202.822/2018 and H.C.C.F.N. grant # E26/210.181/2020).
The authors would like to thank Marcio Marinho Gonzalez for his excellent technical assistance with LDPM recordings and Edson Fernandes de Assis for performing the cytokine assays with the multiplex platform at the Instituto Oswaldo Cruz, Fiocruz, Rio de Janeiro. We would also like to thank Fabiana Muccillo and Renata Carvalho Moreira for technical assistance in the procedures of blood processing and deep-freeze storage.
