
The anecdotal report describes two examples of COVID-19-positive healthcare professionals (HCPs) who had worked as nurses during pre-symptomatic period and subsequently presented a mild clinical course of COVID-19. The nurses’ responsibilities were almost the same and worked in the general ward with no aerosol generating medical procedures. Two HCPs were expected to have similar infectiousness, but the number of secondary transmission by each HCP were different. Eleven close contacts from HCP1 were notified, and all of them tested negative for SARS-CoV-2. However, 13 of 35 close contacts of HCP2 tested positive for SARS-CoV-2. While working, mask-wearing style differed between the two HCPs. HCP1 wore a KF94 mask appropriately and kept wearing it while working.
HCP2 wore a surgical mask while working, but often pulled it down to her chin or removed it. It was strongly suspected that the difference of mask wearing contributed to the SARS-CoV-2 transmission. However, other factors such as talkative behavior, exposure time, ventilation in rooms, and hand hygiene performance rates, could also have affected the transmission of COVID-19.
It is crucial that healthcare workers wear a mask adequately and continuously, and they maintain proper hand hygiene while working during the COVID-19 pandemic.
Asymptomatic and pre-symptomatic transmission of SARS-CoV-2 has been reported.1,2 The virus is mainly transmitted between people through respiratory droplets and close contact.3 Health Care Professionals (HCP) with COVID-19 can infect patients and healthcare co-workers, leading to fatal outcomes. Wearing a mask, social distancing, and hand washing prevent the spread of COVID-19.3 Face masks in particular greatly reduce the risk of coronavirus transmission in public and healthcare settings.4
A 32-year-old woman (HCP1) who had been identified as a close contact tested positive for SARS-CoV-2; mild symptoms developed one day after. During the early infectious period (starting 48 h before the onset of symptoms) she had worked for about nine hours in the hospital without symptoms. While working, she wore a Korean filter 94 mask (KF94 mask) appropriately and continuously, except when she ate (approximately 20 min). Eleven of her close contacts including five patients and six healthcare workers were identified. All of them tested negative for SARS-CoV-2. Moreover, no confirmed COVID-19 cases have been associated with this individual (Table 1).
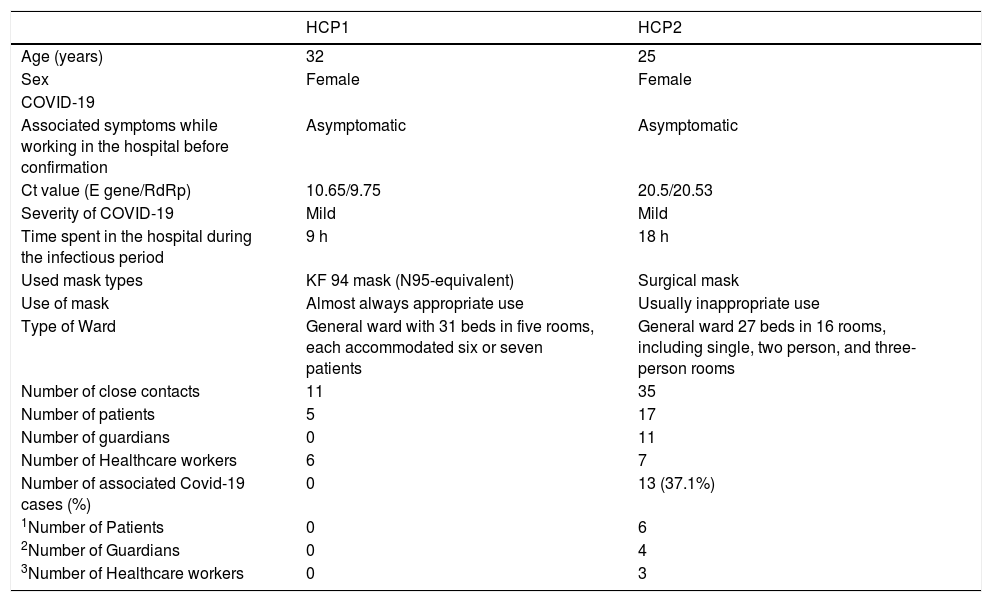
Demographic and clinical characteristics of two HCPs.
| HCP1 | HCP2 | |
|---|---|---|
| Age (years) | 32 | 25 |
| Sex | Female | Female |
| COVID-19 | ||
| Associated symptoms while working in the hospital before confirmation | Asymptomatic | Asymptomatic |
| Ct value (E gene/RdRp) | 10.65/9.75 | 20.5/20.53 |
| Severity of COVID-19 | Mild | Mild |
| Time spent in the hospital during the infectious period | 9 h | 18 h |
| Used mask types | KF 94 mask (N95-equivalent) | Surgical mask |
| Use of mask | Almost always appropriate use | Usually inappropriate use |
| Type of Ward | General ward with 31 beds in five rooms, each accommodated six or seven patients | General ward 27 beds in 16 rooms, including single, two person, and three-person rooms |
| Number of close contacts | 11 | 35 |
| Number of patients | 5 | 17 |
| Number of guardians | 0 | 11 |
| Number of Healthcare workers | 6 | 7 |
| Number of associated Covid-19 cases (%) | 0 | 13 (37.1%) |
| 1Number of Patients | 0 | 6 |
| 2Number of Guardians | 0 | 4 |
| 3Number of Healthcare workers | 0 | 3 |
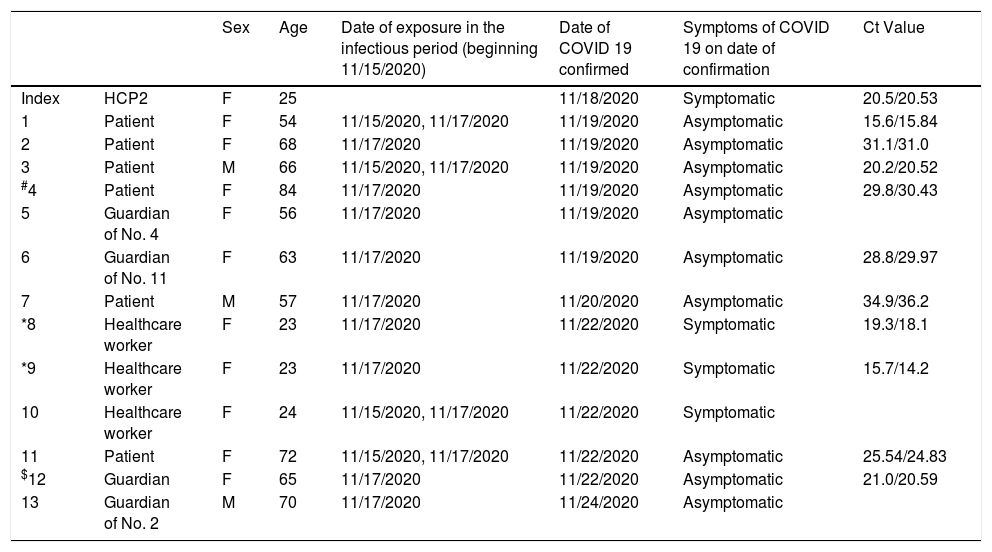
A 25-year-old woman (HCP2) with acute fever tested positive for COVID-19. During the early infectious period she had worked for about 18 h in the hospital without symptoms: nine hours three days and nine hours one day before onset of symptoms. While working, she wore a surgical mask continuously, but often inappropriately, such as pulling it down to her chin. She had been assigned 14 patients and inserted a peripheral venous catheter into one unassigned patient. While working, she had 35 close contacts, including 17 patients, 11 guardians of patients, and seven healthcare workers, all of whom were notified and tested on the same day when the nurse's COVID-19 was confirmed. Six of them tested positive. Subsequently, seven more close contacts turned out to be positive for SARS-CoV-2 (Table 2). This report describes two examples of COVID-19-positive HCPs who had worked as nurses during pre-symptomatic period and subsequently presented a mild clinical course of COVID-19. The COVID-19 prevention policies of the hospital were the same for the two HCPs, as were the nurses’ responsibilities. Two HCPs were expected to have similar infectiousness, but the number of secondary transmission by each HCP were different. In fact, HCP1 had a lower cycle threshold (Ct) value on RT-PCR for SARS-CoV-2 than HCP2. The two HCPs worked in the general ward, but there was a difference in the type of rooms in the ward. The ward in which HCP1 worked had six- or seven-person rooms, whereas the ward in which HCP2 worked had single-, two- and three-person rooms. Therefore, HCP1’s ward was probably more crowded and vulnerable to the spread of infection than HCP’2 ward. When working in the hospital, mask-wearing style differed between the two HCPs. HCP1 wore a KF94 mask appropriately and kept wearing it while working whereas HCP2 wore a surgical mask while working, but often pulled it down to her chin or removed it. A previous report suggested that surgical masks were similar to N95 respirators in preventing COVID-19 especially during non-aerosol generating conditions.5 Moreover, N95 or similar respirators are associated with more discomfort and poorer adherence than surgical mask.5,6 Two HCPs worked in the general word without aerosol generating medical procedures. The appropriateness of mask wearing more likely contributed to the SARS-CoV-2 transmission than type of masks. However, the explanation that the SARS-CoV-2 transmission resulted from the difference in mask wearing could be argued. First, the exposure time was different for the two HCPs. Although the two HCPs had no symptoms when working, HCP2 was exposed repeatedly and for longer periods compared to HCP1. Additionally, talkative behavior, difference in room ventilation, and hand hygiene performance rates are other factors that could have affected transmission of COVID-19.
Clinical characteristics of the patients with COVID-19 after exposure.
| Sex | Age | Date of exposure in the infectious period (beginning 11/15/2020) | Date of COVID 19 confirmed | Symptoms of COVID 19 on date of confirmation | Ct Value | ||
|---|---|---|---|---|---|---|---|
| Index | HCP2 | F | 25 | 11/18/2020 | Symptomatic | 20.5/20.53 | |
| 1 | Patient | F | 54 | 11/15/2020, 11/17/2020 | 11/19/2020 | Asymptomatic | 15.6/15.84 |
| 2 | Patient | F | 68 | 11/17/2020 | 11/19/2020 | Asymptomatic | 31.1/31.0 |
| 3 | Patient | M | 66 | 11/15/2020, 11/17/2020 | 11/19/2020 | Asymptomatic | 20.2/20.52 |
| #4 | Patient | F | 84 | 11/17/2020 | 11/19/2020 | Asymptomatic | 29.8/30.43 |
| 5 | Guardian of No. 4 | F | 56 | 11/17/2020 | 11/19/2020 | Asymptomatic | |
| 6 | Guardian of No. 11 | F | 63 | 11/17/2020 | 11/19/2020 | Asymptomatic | 28.8/29.97 |
| 7 | Patient | M | 57 | 11/17/2020 | 11/20/2020 | Asymptomatic | 34.9/36.2 |
| *8 | Healthcare worker | F | 23 | 11/17/2020 | 11/22/2020 | Symptomatic | 19.3/18.1 |
| *9 | Healthcare worker | F | 23 | 11/17/2020 | 11/22/2020 | Symptomatic | 15.7/14.2 |
| 10 | Healthcare worker | F | 24 | 11/15/2020, 11/17/2020 | 11/22/2020 | Symptomatic | |
| 11 | Patient | F | 72 | 11/15/2020, 11/17/2020 | 11/22/2020 | Asymptomatic | 25.54/24.83 |
| $12 | Guardian | F | 65 | 11/17/2020 | 11/22/2020 | Asymptomatic | 21.0/20.59 |
| 13 | Guardian of No. 2 | M | 70 | 11/17/2020 | 11/24/2020 | Asymptomatic |
Nonetheless, it is crucial that healthcare workers wear a mask adequately and continuously, in addition to maintaining proper hand hygiene while working during the COVID-19 pandemic.
This paper was supported in part by the Foundation of Wonkwang University in 2019.
