

The goal of this study was to determine the prevalence of human papillomavirus infection infection and cervical lesions and its associated factors among HIV infected women attending an AIDS clinic in Amazonas state, Brazil.
MethodsCross-sectional study. Women attending an AIDS clinic in the city of Manaus between March and December 2011 for gynecological examination were invited to participate. Enrolled patients answered a standardized interview including demographical, behavioral, and clinical data. Additionally, patients underwent a gynecological evaluation with collection of cervical samples for cytological analysis and high-risk human papillomavirus infection hybrid capture. A blood sample was also obtained to determine CD4 and viral load levels.
ResultsA total of 310 (82.9%) women participated in the study. High-risk human papillomavirus infection was detected in 191 (61.6%) cases; 24 (13.5%) had low-grade squamous intraepithelial lesion (SIL) and 4 (2.2%) high-grade SIL. No invasive cervical cancer was diagnosed. Median age was 32 (interquartile range (IQR): 27–38) years and median of education was 8.5 (IQR 4–11) years of schooling and 56.1% had a monthly income up to US$180. In multivariate analysis, being less than 30 years old [OR=1.7 (95% CI: 1.2–2.4, p=0.005)], high-grade SIL [OR=6.5 (95% CI: 1.6–23.0, p=0.009)], and CD4 counts <200cells/mm3 [OR=1.6 (95% CI: 1.2–2.0, p<0.001)] were associated with high risk human papillomavirus infection infection.
ConclusionsIn the present study high-risk human papillomavirus infection was frequent and it was associated to high-SIL. These results show the importance of gynecologic examinations in routine care and follow-up required by those who present with cervical lesions.
Although screening for cervical cancer is recommended for women in most countries, with varying age range and periodicity of testing, the incidence of cervical cancer and its related mortality is far greater in developing countries.1 Invasive cervical cancer (ICC) is the second most common cancer in women of childbearing age in Brazil2 and about 15.1% of women in the general population are estimated to be infected by cervical human papillomavirus infection (HPV) in 2012.2 An estimated 15,590 new ICC cases will be diagnosed in Brazil in 2014 (15.33/100,000 women).3
Cervical cancer is the most incident in northern Brazil (23.57/100,000). In the state of Amazonas the ICC is a concern because it has the highest incidence rate estimated in Brazil (630 cases; 35.13/100,000 women) in 2014. In the same year, the capital city of Manaus had an estimated rate of three and a half times greater than that expected for the country besides having the highest incidence rate among Brazilian capitals (510 cases; 53.3/100,000 women).3
The spread of HIV/AIDS in northern Brazil and in the State of Amazonas, in particular, is worrisome especially by the vulnerability of this geographical area, which is determined by the ethnic-cultural diversity of their inhabitants.4,5 The precarious living conditions of the population, and the lack of access to basic needs and health care, given the magnitude of the disease and current epidemiological trends, are important issues in this population, especially regarding hospital beds availability.6
In Brazil the total cumulative cases of AIDS from 1980 to June 2014 was 757,042 cases and 35.0% of this total were women. The mortality rate for women was 4.3/100,000 inhabitants (2013), observing an increase of 3.9 deaths per 100,000 inhabitants in 2004 to 4.3 in 2013. In 2013, the incidence rate of AIDS in the Amazon state was the second largest in the country (37.4/100,000 inhabitants), and the mortality rate for the third largest (8.7/100,000 inhabitants). The capital city of Manaus had the third highest incidence rate of AIDS among all Brazilian capital cities (59.7/100,000 inhabitant), with a mortality rate of 12.5%.7
Women infected by HIV present significantly higher rates of squamous intraepithelial lesions (SIL) and are more susceptible to invasive cervical carcinoma progression than HIV-negative women.8–11 The prevalence of HPV infection is usually greater in HIV-infected women12,13 and it might be explained by the maintenance of high plasma14 and genital15 viral load and persistent HPV infection10,15–17 as a result of HIV infection, which increases the risk to develop SIL.14–18
Wherever HIV-infected women have access and good coverage to cervical cancer screening, they will have better prognosis as a consequence to early diagnosis and treatment of cervical lesions, avoiding progression to cancer. There are not published data focusing on this problem in Amazonas and these results of the present can be used to elaborate prevention strategies for this population. The goal of this study was to evaluate the prevalence of HPV infection and cervical lesions in women infected by HIV attending an AIDS clinic in Manaus, Amazonas, Brazil.
Material and methodsThis was a cross-sectional study conducted among HIV-infected women who attended the AIDS clinic of a tertiary referral hospital in the city of Manaus, Amazonas, Brazil, between March and December 2011. The hospital was the Tropical Medicine Foundation Dr. Heitor Vieira Dourado (FMT-HVD) in the city of Manaus. The total of women infected by HIV registered at FMT-HVD was 2062 cases. In the study period 419 patients, attending the clinic for routine gynecological examination, were invited to participate. In order to be included in the study women had to have a confirmed anti-HIV result, be aged 18–49 years, and agreed to participate. The exclusion criteria were pregnancy at the time of study, previous hysterectomy, or history of cervical conization (Fig. 1).

Enrolled patients answered a face-to-face standardized interview including demographic, behavioral and clinical data, after signing the informed consent form. They also underwent a gynecological evaluation and cervical samples were collected for cytological analysis, which followed the recommendations of the Brazilian Ministry of Health.19 The classification used for cytological results was the Bethesda System for epithelial cell abnormalities – atypical squamous cells of undetermined significance (ASC-US); Cannot exclude HSIL (ASC-H); Low-grade squamous intraepithelial lesion (LSIL); High-grade squamous intraepithelial lesion (HSIL).19 Colposcopic abnormalities were biopisied and submitted to histological analyses. A blood sample was obtained to determine CD4 and viral load levels.
Samples for molecular biology tests were collected prior to the collection for cytology. The test used for detecting HPV-DNA was the (HC2) low (6, 11, 42, 43 e 44) and high risk (HPV 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59 e 68) Hybrid Capture2V2®. The samples were collected using brush-type “cytobrush,” which are part of HC2 (DIGENE®) to microwell hybridization signal amplification by detecting chemiluminescence to qualitatively detect HPV. Hybrid capture was also performed for Chlamydia trachomatis.
Samples were transported in room temperature conditions right after specimen collection or in low temperatures (−2 to 8°C) when there was a delay of up to two days after collection before sending to the Laboratory of Molecular Biology of the FMT-HVD in Manaus, Amazonas.
The primary outcome variable was HPV positivity for lower and/or high-risk genotypes, defined as any positive HC2. To determine factors associated with the prevalence of high risk HPV, predicting variables such as demographic, behavioral, and clinical data were examined. Demographic variables included were state of origin, age in years, years of schooling, marital status, monthly income, and tobacco use. Behavioral variables were age at first sexual intercourse, regular condom use, previous sexual violence, commercial sex work, practice of anal sex, homosexual relationship, illicit drug use, and injecting drug use. Clinical variables were genital bleeding, cervical cytology results and Chlamydia trachomatis test results, CD4 counts and viral load level at HPV diagnosis, as well as infection status (categorized as HIV infection or AIDS).
Data were analyzed using the SPSS 17.0. A preliminary analysis was performed using exploratory techniques. Chi-square tests, Student's t tests and analysis of variance were used. The odds ratio was used as a measure of association, estimated with a 95% confidence interval and those with p<0.05 were considered to be significantly associated with the outcome variable (high-risk HPV). Multivariate analysis was performed to determine variables independently associated the outcome of interest, through the use of logistic regression models. All variables with a p≤0.15 in univariate analyses were included in multivariate analysis.
This study was submitted to and approved by the internal review board of the Amazonas FMT-HVD #327-09/2009. Written consent was given by the patients for their information to be stored in the hospital database and used for research.
ResultsThis study evaluated 419 women, 374 met the eligibility criteria. Eight cases were excluded because of pregnancy, previous hysterectomy, age greater than 49 years old, and duplication of participation. After the interview, 56 women did not undergo sample collection. A total of 310 (82.9%) women were included in the study (Fig. 1). All women were on antiretroviral therapy (ART).
High-risk HPV was detected in 191 (61.6%) cases; 24 (13.5%) had LSIL and four (2.2%) HSIL. There were no cases of invasive cervical cancer.
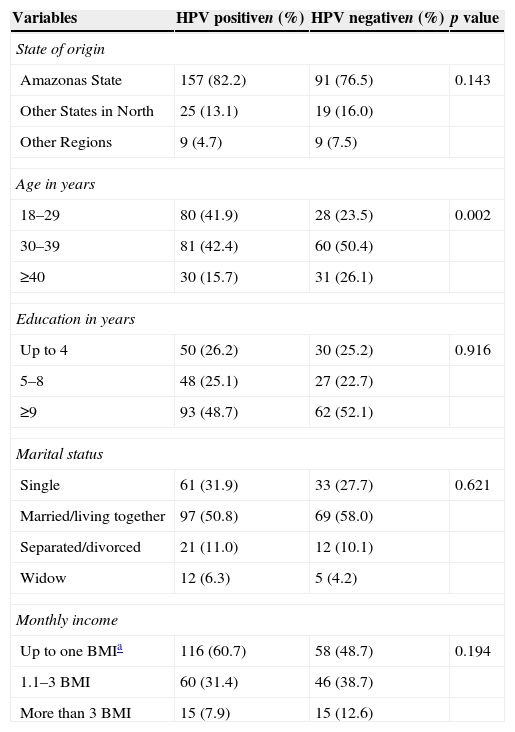
Median age was 32 (interquartile range (IQR): 27–38) years and median of education was 8.5 (IQR 4–11) years of schooling. A total of 56.1% had a monthly income up to US$180. Table 1 shows demographic data; age was the only variable significantly different between groups.
Demographical characteristics of the 310 participants HIV women, attendees of the service of specialized care for AIDS in Manaus, Amazonas, Brazil.
| Variables | HPV positiven (%) | HPV negativen (%) | p value |
|---|---|---|---|
| State of origin | |||
| Amazonas State | 157 (82.2) | 91 (76.5) | 0.143 |
| Other States in North | 25 (13.1) | 19 (16.0) | |
| Other Regions | 9 (4.7) | 9 (7.5) | |
| Age in years | |||
| 18–29 | 80 (41.9) | 28 (23.5) | 0.002 |
| 30–39 | 81 (42.4) | 60 (50.4) | |
| ≥40 | 30 (15.7) | 31 (26.1) | |
| Education in years | |||
| Up to 4 | 50 (26.2) | 30 (25.2) | 0.916 |
| 5–8 | 48 (25.1) | 27 (22.7) | |
| ≥9 | 93 (48.7) | 62 (52.1) | |
| Marital status | |||
| Single | 61 (31.9) | 33 (27.7) | 0.621 |
| Married/living together | 97 (50.8) | 69 (58.0) | |
| Separated/divorced | 21 (11.0) | 12 (10.1) | |
| Widow | 12 (6.3) | 5 (4.2) | |
| Monthly income | |||
| Up to one BMIa | 116 (60.7) | 58 (48.7) | 0.194 |
| 1.1–3 BMI | 60 (31.4) | 46 (38.7) | |
| More than 3 BMI | 15 (7.9) | 15 (12.6) | |
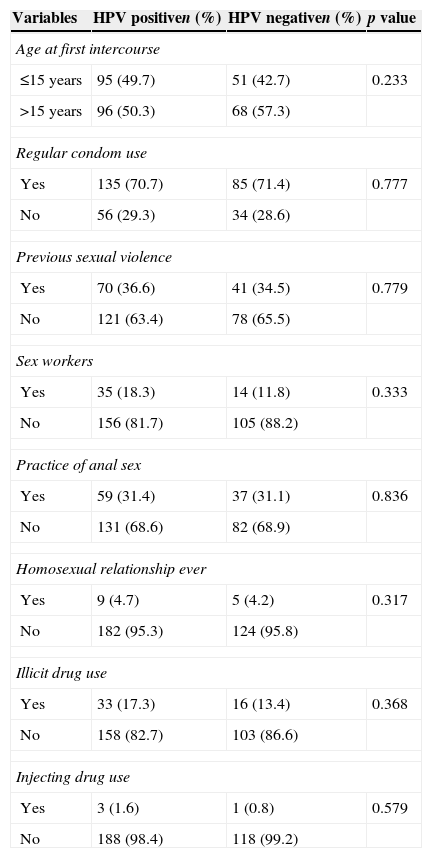
Behavioral features are described in Table 2: 9.7% were tobacco users, 49 (15.8%) illicit drug abusers, 220 (71.0%) used condoms regularly in last year, and 49 (15.8%) were commercial sex workers. There was no difference between the two groups.
Behavior characteristics of the 310 participants HIV women, attendees of the service of specialized care for AIDS in Manaus, Amazonas, Brazil.
| Variables | HPV positiven (%) | HPV negativen (%) | p value |
|---|---|---|---|
| Age at first intercourse | |||
| ≤15 years | 95 (49.7) | 51 (42.7) | 0.233 |
| >15 years | 96 (50.3) | 68 (57.3) | |
| Regular condom use | |||
| Yes | 135 (70.7) | 85 (71.4) | 0.777 |
| No | 56 (29.3) | 34 (28.6) | |
| Previous sexual violence | |||
| Yes | 70 (36.6) | 41 (34.5) | 0.779 |
| No | 121 (63.4) | 78 (65.5) | |
| Sex workers | |||
| Yes | 35 (18.3) | 14 (11.8) | 0.333 |
| No | 156 (81.7) | 105 (88.2) | |
| Practice of anal sex | |||
| Yes | 59 (31.4) | 37 (31.1) | 0.836 |
| No | 131 (68.6) | 82 (68.9) | |
| Homosexual relationship ever | |||
| Yes | 9 (4.7) | 5 (4.2) | 0.317 |
| No | 182 (95.3) | 124 (95.8) | |
| Illicit drug use | |||
| Yes | 33 (17.3) | 16 (13.4) | 0.368 |
| No | 158 (82.7) | 103 (86.6) | |
| Injecting drug use | |||
| Yes | 3 (1.6) | 1 (0.8) | 0.579 |
| No | 188 (98.4) | 118 (99.2) | |
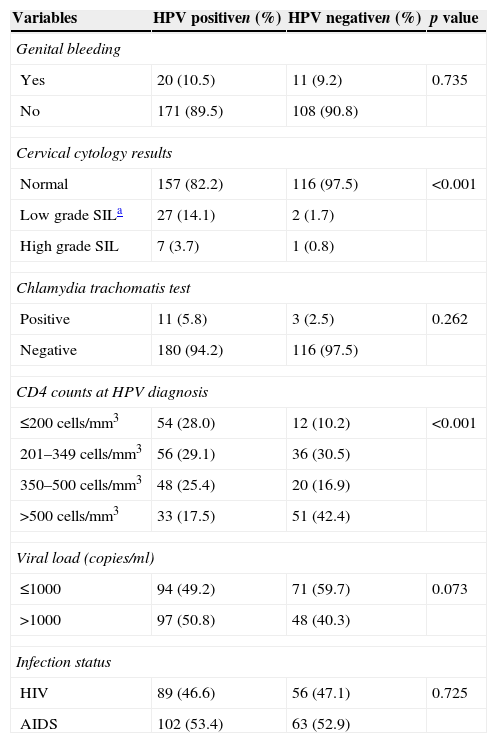
The median of CD4+T cell counts and of viral load was 338.5 (IQR=211.5–513.3)cells/mm3 and 497.5 (IQR=49–11,288) copies/mm3 respectively. A total of 165 (53.2%) HIV infected women were classified as patients with AIDS. The HPV infected women were different from HPV uninfected group regarding CD4 count less than 200 (28% vs. 10.2%, p<0.001) and HSIL (3.7% vs. 0.8%, p=0.001). Clinical data are described in Table 3.
Clinical characteristics of the 310 participants HIV women, attendees of the service of specialized care for AIDS in Manaus, Amazonas, Brazil.
| Variables | HPV positiven (%) | HPV negativen (%) | p value |
|---|---|---|---|
| Genital bleeding | |||
| Yes | 20 (10.5) | 11 (9.2) | 0.735 |
| No | 171 (89.5) | 108 (90.8) | |
| Cervical cytology results | |||
| Normal | 157 (82.2) | 116 (97.5) | <0.001 |
| Low grade SILa | 27 (14.1) | 2 (1.7) | |
| High grade SIL | 7 (3.7) | 1 (0.8) | |
| Chlamydia trachomatis test | |||
| Positive | 11 (5.8) | 3 (2.5) | 0.262 |
| Negative | 180 (94.2) | 116 (97.5) | |
| CD4 counts at HPV diagnosis | |||
| ≤200cells/mm3 | 54 (28.0) | 12 (10.2) | <0.001 |
| 201–349cells/mm3 | 56 (29.1) | 36 (30.5) | |
| 350–500cells/mm3 | 48 (25.4) | 20 (16.9) | |
| >500cells/mm3 | 33 (17.5) | 51 (42.4) | |
| Viral load (copies/ml) | |||
| ≤1000 | 94 (49.2) | 71 (59.7) | 0.073 |
| >1000 | 97 (50.8) | 48 (40.3) | |
| Infection status | |||
| HIV | 89 (46.6) | 56 (47.1) | 0.725 |
| AIDS | 102 (53.4) | 63 (52.9) | |
In multivariate analysis, being less than 30 years old [OR=1.7 (95% CI: 1.2–2.4, p=0.005)], HSIL [OR=6.5 (95% CI: 1.6–23.0, p=0.009)], and CD4 count <200cells/mm3 [OR=1.6 (95% CI: 1.2–2.0, p<0.001)] were associated with high risk HPV infection in the final model.
DiscussionThis study found a high prevalence of high risk HPV in HIV infected women in Manaus. These results underscore the importance of routine gynecologic examinations and follow-up in those who present with cervical lesions. These results are in agreement with other Brazilian10,20–23 and international studies12–14,24,25 that showed high prevalence of high risk HPV among HIV infected women.
It is important to emphasize that it was found low prevalence of HSIL in this group and there was no invasive cervical cancer. These findings could be explained by the high rate of ART use and by the higher access of HIV infected women to gynecological care in Brazil. As they go to the clinic to be followed for the HIV infection they are also more frequently submitted to pap smear and can therefore be diagnosed earlier.
HPV is considered one of the most important risk factors for cervical cancer.26–28 In the present study high risk HPV was associated to HSIL. HPV infection and SIL are common in HIV infected women,12–14,29–31 who may be asymptomatic. As HIV infected women may have faster progression, all women with SIL must be tested for HIV, because it might be a signal of immunosuppression.14,31 Factors related to HPV infection also contribute to progression of the infection to cancer, such as HPV genotype, viral variants, persistence of infection, and viral load.15,32,33 The high-risk types are more likely to cause persistent lesions and be associated with precancerous lesions.25,34
Other associated factor with high risk HPV in this study was lower CD4 lymphocyte cells counting (<200cell/mm3). Other studies suggested that the frequency of HPV persistence varied inversely with CD4+ count, and found higher HPV prevalence and incidence of oncogenic HPV types in HIV infected patients, especially those with lower CD4+ counts.13,18,31 These data suggest that the level of CD4 is important in the pathogenesis of HPV infection in HIV infected patients.25,31
Cross-sectional studies can be carried out to investigate associations between risk factors and the outcome of interest. They are limited, however, by the fact that they are carried out at one time point and give no indication of the sequence of events. For this reason, it is impossible to infer causality. Its application is justified in this study for assessing the prevalence of and the associated factors for high risk HPV among HIV infected women. It is important to demonstrate the susceptibility of this group of women to the complications of this infection. In this study, the possibility of response bias could not be ruled out. There is always a general tendency to give socially acceptable answers.
Performing routinely cervical cytological exam is recommended25,35 and in case of any degree of abnormality in this evaluation women should be referred to colposcopy assessment.36–38 HIV-infected women with cervical invasive carcinoma normally present faster evolution and greater chance for disease recurrence.13 Cervical cancer incidence in HIV-infected women is not altered by use of ARV therapy.27,38 Therapeutic management is the same as for uninfected women, irrespective of HIV serology,35 but with poorer prognosis in women with AIDS.26,35
Cancer prevention programs exist and have been shown to be successful at avoiding disease progression among women infected by HIV. Although this is encouraging, much work still remains in order to identify additional innovative interventions that address social, cultural, and environmental influences of HPV infection and cervical cancer. There is also a need to find better ways of disseminating evidence-based approaches to HIV prevention, so that effective interventions are more widely used.35
In conclusion, it was demonstrated high prevalence of high-risk HPV infection in women living with HIV in Manaus, being significantly associated with age less than 30 years old, presence of high-grade SIL and CD4 counts <200cells/mm3. In cities of the Brazilian Amazon, access to sexual and reproductive care, contribute effectively to prevent lesions and cervical cancer in this population.
Conflicts of interestThe authors declare no conflicts of interest.
The team would like to thank the International Clinical, Operational, and Health Services Research and Training Award (ICOHRTA) Program, the Fogarty International Center/US National Institutes of Health # U2RTW006885 ICOHRTA-NIH AI066994 for grant support.
