
Itajaí is a port city in southern Brazil with one of the highest incidence and mortality rates from AIDS in the country. The prevalence and incidence of HIV infection were investigated in 1085 of 3196 new HIV-1 infection cases evaluated in the counseling and testing center of Itajaí from January 2002 to August 2008. Recent infections were assessed using the BED™, and pol region sequencing was performed in 76 samples. The prevalence ranged from 3.08% to 6.17% among women and from 10.26% to 17.36% among men. A total of 17% of infections were classified as recent, with annual incidence varying from 1.6% to 4.8 per 100 patient/year among women and from 2.05% to 8.5 per 100 patient/year among men. Pol sequences were obtained from 38 randomly recent infections selected individuals: 71% were infected by subtype C, 24% B, 2% D, and 2% F1. Among 38 subjects with established infection, 76% were subtype C, and 24% B. Transmitted drug resistance was detected in 18.4% of recent infection subjects (7.8% to nucleoside analog reverse-transcriptase inhibitors, 5.2% to non-nucleoside reverse-transcriptase inhibitors, and 5.2% protease inhibitors) and 5.2% of subjects with established infection had nucleoside analog reverse-transcriptase inhibitors resistance.
The high prevalence and incidence of HIV infection in this region is unprecedented in studies involving cases evaluated in the counseling and testing centers in Brazil.
From 1982 to June 2012, 656,701 cases of AIDS were reported in Brazil.1 Brazil is divided into five macroregions: north, northeast, midwest, southeast, and south. The southeast and south regions are the most economically developed and have the highest number of AIDS cases in the country. In contrast, the mortality rate from AIDS is higher in the poorer regions of the country.1 An interesting peculiarity has been reported in Itajaí, a city located in the state of Santa Catarina in southern Brazil. This port city, with approximately 185,000 inhabitants, often leads the ranks in the number of AIDS cases per 100,000 inhabitants2 and of mortality rates from AIDS.1
Several studies have been conducted in Brazil to evaluate the genetic diversity of HIV-1 in the country and have revealed the presence of subtypes B, F, C, and a significant number of recombinant subtypes.3,4 Subtype B virus is the most prevalent throughout the country, whereas subtype C virus and its recombinant forms are highly prevalent in southern Brazil.3,4 The prevalence of transmitted drug resistance (TDR) to antiretroviral agents in Brazil is considered moderate, typically ranging from 5% to 10%.5
In this study, we analyzed the prevalence and incidence of HIV-1 infection in a counseling and testing center (CTC) in Itajaí to gain further insight into the high incidence of AIDS and high HIV-related mortality.
Materials and methodsThis is a retrospective analysis evaluating stored sera samples and data registered in medical files. From January 2002 to August 2008, we evaluated 1085 patients from the CTC in Itajaí who were diagnosed with HIV-1. The patients had never used antiretroviral drugs, and HIV serology was confirmed with two ELISA tests and western blotting. Serum samples were sent to the Retrovirology Laboratory at the Federal University of São Paulo, where further laboratory tests were performed. The study was approved by the Institution's Research Ethics Committee.
To determine recent infection (RI), the AWARE™ BED™ EIA HIV-1 incidence test was used according to the manufacturer's instructions, and the incidence was calculated according to previously established guidelines.6
To determine the HIV-1 subtypes and the occurrence of TDR, 38 samples were randomly selected from subjects with RI and 38 samples from subjects with established infection (EI). All samples were processed as previously described.7 TDR was evaluated according to an algorithm that excludes common polymorphisms.8 The profile of HIV-1 subtypes was determined using REGA HIV-1 Subtyping tool version 2.0 (http://www.bioafrica.net/rega-genotype/html/index.html).
For statistical analysis, calculations were performed to determine the prevalence and estimated incidence rates of infection.6 Moreover, parametric and nonparametric distribution tests, as well as descriptive analyses, were performed.
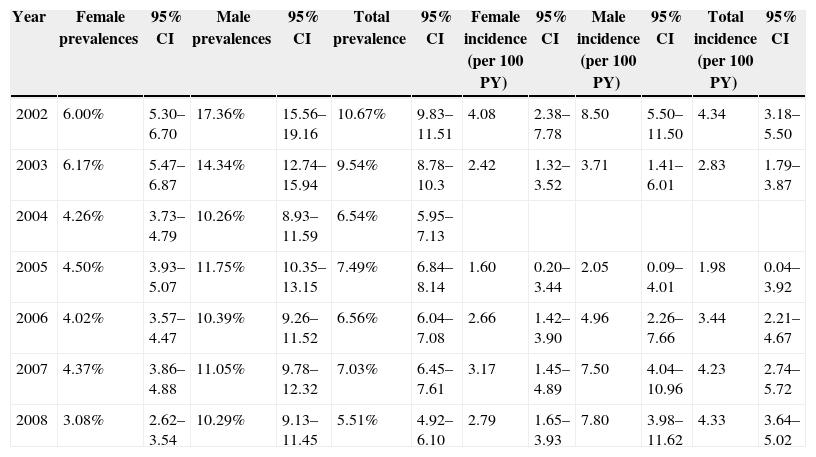
ResultsBetween January 2002 and August 2008, 41,115 subjects visited the CTC in Itajaí. Among them, 3196 subjects had positive HIV serology, and 1085 subjects were enrolled in the study. The prevalence and incidence rates of HIV infection according to year and gender are shown in Table 1.
Prevalence and incidence among males and females from 2002 to 2008.
| Year | Female prevalences | 95% CI | Male prevalences | 95% CI | Total prevalence | 95% CI | Female incidence (per 100 PY) | 95% CI | Male incidence (per 100 PY) | 95% CI | Total incidence (per 100 PY) | 95% CI |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 2002 | 6.00% | 5.30–6.70 | 17.36% | 15.56–19.16 | 10.67% | 9.83–11.51 | 4.08 | 2.38–7.78 | 8.50 | 5.50–11.50 | 4.34 | 3.18–5.50 |
| 2003 | 6.17% | 5.47–6.87 | 14.34% | 12.74–15.94 | 9.54% | 8.78–10.3 | 2.42 | 1.32–3.52 | 3.71 | 1.41–6.01 | 2.83 | 1.79–3.87 |
| 2004 | 4.26% | 3.73–4.79 | 10.26% | 8.93–11.59 | 6.54% | 5.95–7.13 | ||||||
| 2005 | 4.50% | 3.93–5.07 | 11.75% | 10.35–13.15 | 7.49% | 6.84–8.14 | 1.60 | 0.20–3.44 | 2.05 | 0.09–4.01 | 1.98 | 0.04–3.92 |
| 2006 | 4.02% | 3.57–4.47 | 10.39% | 9.26–11.52 | 6.56% | 6.04–7.08 | 2.66 | 1.42–3.90 | 4.96 | 2.26–7.66 | 3.44 | 2.21–4.67 |
| 2007 | 4.37% | 3.86–4.88 | 11.05% | 9.78–12.32 | 7.03% | 6.45–7.61 | 3.17 | 1.45–4.89 | 7.50 | 4.04–10.96 | 4.23 | 2.74–5.72 |
| 2008 | 3.08% | 2.62–3.54 | 10.29% | 9.13–11.45 | 5.51% | 4.92–6.10 | 2.79 | 1.65–3.93 | 7.80 | 3.98–11.62 | 4.33 | 3.64–5.02 |
CI, confidence interval.
New cases of HIV-1 infection during the study period were diagnosed through serological testing of the biological material provided by the CTC in Itajaí, state of Santa Catarina (SC). Male/female ratios obtained were 1.4:1 in 2002, 1:1 in 2003, 1:1 in 2004, 1.3:1 in 2005, 1.2:1 in 2006, 1.2:1 in 2007, and 1.4:1 in 2008. In 2008, the ratio was estimated proportionately because data were collected only until August.
Of the 1085 patients enrolled in the study, 519 (48%) were women, among whom 40 (8%) were pregnant. Their age ranged from 1.8 to 76 years, with a mean age of 34.90±11.16 years and a median age of 34 years.
Regarding sexual orientation, 834 (81%) subjects were heterosexuals, 35 (3%) male homosexuals, 14 (1%) bisexual, and 150 (15%) did not answer the question. Furthermore, 785 (72%) subjects reported having acquired HIV through sexual intercourse: 33 (3%) through blood transfusion, 63 (6%) through injection drug use (IDU), 44 (4%) by vertical transmission, 2 (0.2%) through exposure to HIV-contaminated biological material, and 156 (14%) did not answer the question. Regarding the number of sexual partners per year, 10 (1%) respondents reported having no partners in the last year; 626 (61%) had 1 partner; 21 (1%) had 2 partners; 106 (10%) had 3 partners; 36 (3%) had 4–10 partners; 30 (3%) had more than 10 partners; and 204 (20%) did not answer the question. Regarding use of condoms, 488 (62%) reported not having used condoms; 148 (19%) reported sporadic use; 104 (13%) reported use of condoms in all sexual relations; and 45 (6%) did not answer the question.
Concerning HIV-1 subtypes among people with RI, 9 subjects (24%) were infected by subtype B, 27 (71%) by subtype C, 1 (2%) by subtype D, and 1 (2%) by subtype F1. Among the subjects with EI, 9 (24%) were infected by subtype B, and 29 (76%) by subtype C.
The prevalence of TDR was 18.4% (7 subjects, 95% CI: 8.3–34.9) among subjects with RI, of which 3 (7.8%) subjects had virus resistant to nucleoside reverse transcriptase inhibitors (NRTI; including mutations M41L, T215S, D67N, K70R, K219Q, and L210W), 2 (5.2%) were infected by virus resistant to non-nucleoside reverse transcriptase inhibitors (NNRTI; mutations Y181C and G190E), and 2 (5.2%) had viral resistant to protease inhibitors (PI; mutations V82A and I47V). Among subjects with EI, the prevalence of TDR was 5.2% (2 subjects, 95% CI: 0.9–19.1), both of which had resistance to NRTI (mutations M41L, T215S, D67N, T69D, and K219Q).
There were no significant gender, age, level of education, epidemiology of HIV acquisition, HIV subtypes, and TDR differences.
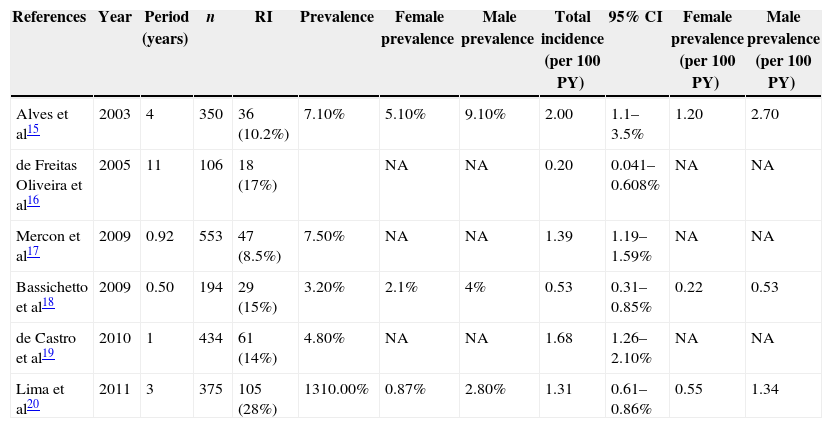
DiscussionThis study reports an unprecedented high prevalence and incidence rates of HIV infection in Brazil (Table 2). Furthermore, it corroborates important findings regarding the feminization of the HIV epidemic in the country. It has been reported that, in general, the ratio of infected men/infected women has decreased from 26.3/1 in the mid-1980s to approximately 1.5/1 in more recent years.1
Prevalence and incidence studies among Brazilian populations using incidence HIV-1 assays.
| References | Year | Period (years) | n | RI | Prevalence | Female prevalence | Male prevalence | Total incidence (per 100 PY) | 95% CI | Female prevalence (per 100 PY) | Male prevalence (per 100 PY) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Alves et al15 | 2003 | 4 | 350 | 36 (10.2%) | 7.10% | 5.10% | 9.10% | 2.00 | 1.1–3.5% | 1.20 | 2.70 |
| de Freitas Oliveira et al16 | 2005 | 11 | 106 | 18 (17%) | NA | NA | 0.20 | 0.041–0.608% | NA | NA | |
| Mercon et al17 | 2009 | 0.92 | 553 | 47 (8.5%) | 7.50% | NA | NA | 1.39 | 1.19–1.59% | NA | NA |
| Bassichetto et al18 | 2009 | 0.50 | 194 | 29 (15%) | 3.20% | 2.1% | 4% | 0.53 | 0.31–0.85% | 0.22 | 0.53 |
| de Castro et al19 | 2010 | 1 | 434 | 61 (14%) | 4.80% | NA | NA | 1.68 | 1.26–2.10% | NA | NA |
| Lima et al20 | 2011 | 3 | 375 | 105 (28%) | 1310.00% | 0.87% | 2.80% | 1.31 | 0.61–0.86% | 0.55 | 1.34 |
Overall, the demographic profile of the subjects being evaluated in the CTC of Itajaí is similar to that found in other existing CTCs in Brazil (data not shown). The subtype profile of the study group revealed a high prevalence of subtype C virus, which is in agreement with previous studies, demonstrating the high prevalence of this subtype in southern Brazil.3 Similarly, the prevalence of TDR and the mutation profile in this small sample are in line with previous studies conducted in other regions of Brazil.5
We acknowledge that tests for detecting recent infections, such as the BED assay, may eventually present flaws6,9–11 and validation studies using subtype C virus are scarce.12–14 Moreover, we recognize that the number of subjects tested to determine viral subtypes and TDR was limited in this study. However, it is of note that the high prevalence and incidence rates of HIV-1 infection in Itajaí, a city with a known high prevalence of AIDS and HIV-related mortality, is unprecedented in Brazil. Therefore, efforts should be made to identify the causes of the problem, decrease the mortality rate from AIDS, and interrupt the transmission cycle. Furthermore, the profile of subjects with recent HIV-1 infection should be better characterized.
Conflicts of interestThe authors declare no conflicts of interest.
