

Respiratory viruses are the major putative agents in infants and children with acute respiratory tract infections (ARTIs). The prevalence and clinical characteristics of acute respiratory tract infections among children in China have been previously reported. However, those surveys were conducted mostly in developed cities, such as Beijing,1 Shanghai,2 Guangzhou,3 and Shenzhen.4 Limited data on pediatric patients with various respiratory viruses were available in medium or small-sized cities in China. This study aims to determine the epidemiological characteristics of seven respiratory viruses (including Influenza A virus, InfA; Influenza B virus, InfB; Respiratory syncytial virus, RSV; Adenovirus, ADV; Parainfluenza virus type 1/2/3, PIV 1/2/3) among children (0–14 years old) presenting with ARTIs between June 2011 and September 2015 in Dongguan, southern China.
In the study, a total of 8031 samples from nasopharyngeal swabs were collected from children with ARTIs at the Children's Hospital of Dongguan. ARTIs were diagnosed according to the Chinese guidelines. This study was approved by the Ethics Committee of Children's Hospital of Dongguan. All patients’ parents provided written informed consent. Seven respiratory viruses were tested by using D3 Ultra DFA Respiratory Virus Screening & ID Kit, Ohio, USA. All procedures were conducted in accordance with the manufactures’ manual.
Of the 8031 enrolled patients, 1867 (23.2%) were positive for at least one virus, and other children with ARTIs might have been infected by other respiratory viruses or microorganisms, such as mycoplasma, chlamydia and bacteria, which were not tested in our study. The positive rate of the seven respiratory viruses was higher than that reported in Shenzhen (4346/30,443, 14.3%)4 and Wuhan (5194/39,756, 13.1%),5 but lower than positivity rate found in Guangzhou (1482/4242, 34.9%).3 The discrepancy might be due to different sample size, varied climate, geographic location, and sensitivity of different detection methods.
RSV (11.8%, 949/8031) was the most frequently detected virus causing ARTIs in this study, which was frequently identified among children less than two years old, notably less than six months of age (Table 1). This was consistent with previous domestic and foreign studies. RSV infection occurred throughout the year, but the high-incidence period was from winter to spring and from summer to autumn in our study. The seasonal changes affecting the prevalence of RSV infection were similar to that in Guangzhou,3 but were different from Beijing (winter),1 Shanghai (winter),2 and Wuhan (winter).5 These findings suggest that seasonal distribution of RSV infection might be associated to geographic locations and meteorology.
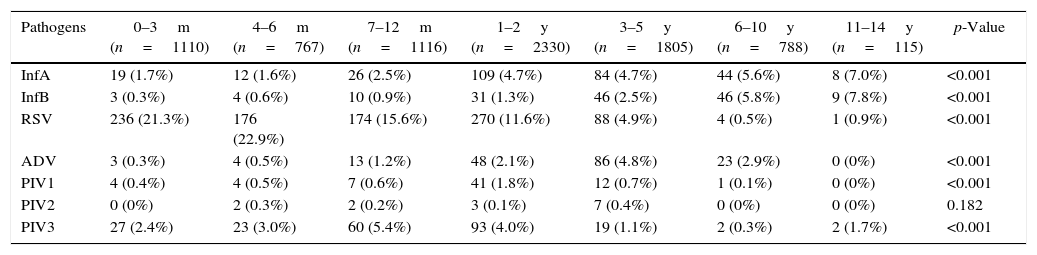
Pathogen positivity rates among patients in different age groups.
| Pathogens | 0–3m (n=1110) | 4–6m (n=767) | 7–12m (n=1116) | 1–2y (n=2330) | 3–5y (n=1805) | 6–10y (n=788) | 11–14y (n=115) | p-Value |
|---|---|---|---|---|---|---|---|---|
| InfA | 19 (1.7%) | 12 (1.6%) | 26 (2.5%) | 109 (4.7%) | 84 (4.7%) | 44 (5.6%) | 8 (7.0%) | <0.001 |
| InfB | 3 (0.3%) | 4 (0.6%) | 10 (0.9%) | 31 (1.3%) | 46 (2.5%) | 46 (5.8%) | 9 (7.8%) | <0.001 |
| RSV | 236 (21.3%) | 176 (22.9%) | 174 (15.6%) | 270 (11.6%) | 88 (4.9%) | 4 (0.5%) | 1 (0.9%) | <0.001 |
| ADV | 3 (0.3%) | 4 (0.5%) | 13 (1.2%) | 48 (2.1%) | 86 (4.8%) | 23 (2.9%) | 0 (0%) | <0.001 |
| PIV1 | 4 (0.4%) | 4 (0.5%) | 7 (0.6%) | 41 (1.8%) | 12 (0.7%) | 1 (0.1%) | 0 (0%) | <0.001 |
| PIV2 | 0 (0%) | 2 (0.3%) | 2 (0.2%) | 3 (0.1%) | 7 (0.4%) | 0 (0%) | 0 (0%) | 0.182 |
| PIV3 | 27 (2.4%) | 23 (3.0%) | 60 (5.4%) | 93 (4.0%) | 19 (1.1%) | 2 (0.3%) | 2 (1.7%) | <0.001 |
Influenza virus was the second most frequently discovered pathogen, including InfA (3.76%, 302/8031) and InfB (1.86%, 149/8031), with the infection rates increasing with age (from 0 to 14 years) (Table 1). The results were concordant with the previous study in Guangzhou.3 Interestingly, the seasonal distribution of InfA infection was different from InfB infection in the current study. InfA was frequently detected in spring and summer, whereas InfB was mostly detected in winter (Fig. 1A). The seasonal distribution of InfA infection was slightly different from other studies in Shenzhen4 and Shanghai.2
 Seasonal distribution of FluA and FluB. (B) Seasonal distribution of RSV and ADV. (C) Seasonal distribution of PIV1-3.")
A total of 177 (2.2%) ADV infected patients had been identified, which was most frequently detected in patients aged 3–5 years (Table 1). The age distribution was not in line with that reported in Shenzhen (peak age 1–3 years)4 and Shanghai (peak age >6 years).2 These differences might have been due to the distribution of different ADV serotypes in above cities. Additionally, the seasonal distribution of ADV infection was not obvious and sometimes diagnosed throughout the year (Fig. 1B), which was consistent with a study from Guangzhou,3 but was different from reports from Shenzhen (winter)4 and Wuhan (spring and winter).5
There were 309 children infected with PIVs, including PIV1 (0.9%, 69/8031), PIV2 (0.2%, 14/8031) and PIV3 (2.8%, 226/8031), which were mostly found in children aged 7–12 months (Table 1). This was different from studies in Guangzhou (peak age 3–6 months)3 and Wuhan (peak age 3–6 years).5 Due to the limited number of PIV1 and PIV2 infections in this study, their seasonal distributions were unclear. PIV3 infection occurred nearly throughout the year, and the seasonal peak was similar to RSV infection.
Additionally, our results showed that co-infections were relatively uncommon in Dongguan, detected only 1.02% (19/1867). It could be attributed to the limited number of pathogens included in the study and the lack of sensitivity of DFA method comparing with PCR method.
Conflicts of interestThe authors declare no conflicts of interest.
This work was supported by the Natural Science Foundation of Guangdong Province (Project Number: 2015A030313803), the Dongguan Bureau of Science and Technology for the City Key Program of Science and Technology (Project Number: 2014108101028) and the Dongguan Bureau of Science and Technology for the City Key Program of Science and Technology (Project Number: 2013108101017). We also thank all the children and their parents for their cooperation during this work.
