





Rifampicin is used in both phases of treatment for tuberculosis. In chronic use, the short half-life and the self-induction of metabolism can decrease the levels of the drug below the minimal inhibitory concentration. The aim of the study was to investigate whether plasma concentrations of rifampicin are sustained above 0.5μg/mL in patients with tuberculosis using 600mg/day. Rifampicin was measured in plasma by high-performance liquid chromatography and a sputum smear microscopy was performed in all days of the study. A total of 44 male patients completed the study. On days 31, 61 and 91, the mean plasma concentrations of rifampicin were 0.6 (0.5)μg/mL, 0.55 (0.5)μg/mL and 0.46 (0.4)μg/mL. There was a high variation of rifampicin levels leading to a high percentage of samples with concentrations below 0.5μg/mL. There was no significant association between the frequency of samples with drug levels below 0.5μg/mL with the conversion of the sputum microscopy. These data suggest that pre-doses samples offer limited information on the exposure of M. tuberculosis to rifampicin.
Tuberculosis is a relevant health issue in Brazil with about 70,000 new cases diagnosed each year. The treatment comprises a fixed-dose combination of rifampicin, isoniazid, pyrazinamide, and ethambutol (RHZE) in the intensive phase and rifampicin with isoniazid (RH) in the continuation phase. Rifampicin is a hydrazone of a rifamycin B derivative with N-amino-N′-methyl piperazine approved by the Food and Drug Administration for treatment of the disease since 1971.1–3
The time of exposure of M. tuberculosis to rifampicin concentrations above the MIC (0.25–0.5μg/mL for wild-type of Mycobacterium) is the best determinant of patient outcome.4,5 However, there is a high variation in rifampicin plasma concentrations after therapeutic doses, which is related to the patients (age, sex, weight, ethnicity, malabsorption, comorbidity, compliance with prescribed regimen, genetic polymorphism of drug metabolizing enzymes and transporters), as well as to the drug administered (quality of the drug dispensed and drug formulation). As a result, adequate exposure of M. tuberculosis to the drug promoting detrimental impact on outcome can be impaired, such as treatment failure, relapse of infection and emergence of resistance.3,6–8
Chronic use of rifampicin increases the rate of disappearance of the drug from blood in the early phase of the treatment with a consequent reduction of its half-life as well as of drug exposure, which is related to its short half-life and self-induction of metabolism.3,9 The objective of the current study was to investigate whether the concentrations of rifampicin in plasma are sustained above the MIC in pre-dose samples collected in both phases of treatment in Brazilian patients with pulmonary tuberculosis on chronic use of daily doses of 600mg of the drug.
This was a prospective study carried out between January 2017 and July 2018 in cases of pulmonary tuberculosis receiving care at the Health Unit of Guama District, City of Belem, PA, Brazil. The inclusion criteria were adult male patients with clinical, laboratory and radiological diagnosis of pulmonary tuberculosis. Exclusion criteria were use of anti-tuberculosis drugs in the last 30 days, cases of retreatment, children, and those coinfected with HIV, hepatitis A, B, C or E viruses, drug addiction including ethanol and tobacco, diabetes mellitus, hepatic or renal diseases, or those with a history of allergy to anti-tuberculosis drugs. Each patient received a daily total dose of rifampicin (600mg), isoniazid (300mg) pyrazinamide (1600mg) and ethambutol (1100mg) for two months (intensive phase), followed by rifampicin (600mg) plus isoniazid (300mg) for four months (continuation phase).10 In the intensive phase, the drugs were dispensed as fixed-dose combination containing rifampicin (150mg), isoniazid (75mg), pyrazinamide (400mg), and ethambutol (275mg). In the continuation phase, the drugs were dispensed as fixed-dose combination containing rifampicin (300mg) and isoniazid (150mg). Both formulations were from the same batch and were provided and analyzed by Farmanguinhos (Fiocruz, Rio de Janeiro, Brazil). The clinical staff of the tuberculosis program from the basic health unit was responsible for prescribing and dispensing the drugs. The patients and their relatives received specific instructions about the administration on each day and were strongly recommended to complete the course of treatment. Patients were requested to return for follow-up monthly on two occasions: in the first, they were clinically evaluated, received the monthly doses of the drugs and the research team supervised the administration of the first monthly dose. In a second occasion, the patients were requested to return to the health unit 24h after the directly observed dose and before the next dose for blood sampling and sputum smear for microscopy on days 31, 61 and 91.
Rifampicin was measured by high-performance liquid chromatography using a Flexar® system (Perkin Elmer), after liquid–liquid extraction from plasma, following the procedure proposed by Zhou et al. (2010) with modifications.11 The mobile-phase was acetonitrile:phosphate buffer pH 3.0 (40:60 v/v) at a flow of 1mL/min and the column was an RP18, 150mm×4.5mm (Perkin Elmer) at 30°C. The eluent was monitored at 254nm. The limit of detection was 0.01μg/mL and the limit of quantification was 0.02μg/mL. The method was linear from 0.02μg/mL to 2μg/mL. The within and the between days variability were 12% and 16% and the mean recovery was 90%.
Qualitative data are presented as frequencies of occurrence and the concentrations of rifampicin in plasma as mean with 95% confidence interval. Categorical variables were compared by chi-squared test. One-way analysis of variance was used to compare the concentrations of rifampicin in plasma among days of blood sampling. Data were analyzed using SPSS software, release 21 (IBM Inc, Chicago, IL, EUA). The significance level was 5%.
The study protocol was revised and approved by the Ethics Committee of the Nucleo de Medicina Tropical da Universidade Federal do Pará (Brazil), under number 1.591.019. All patients gave written consent before inclusion in the study.
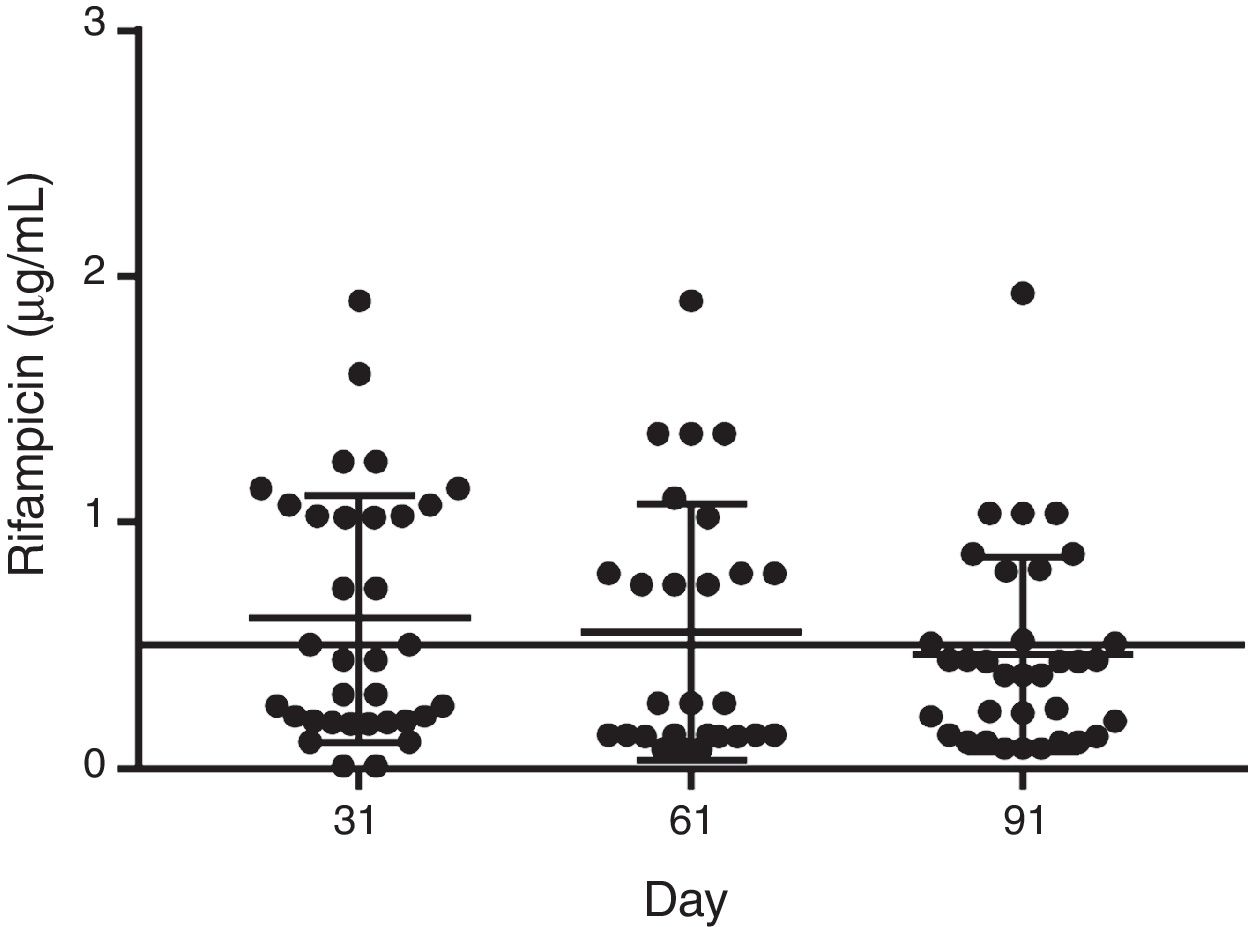
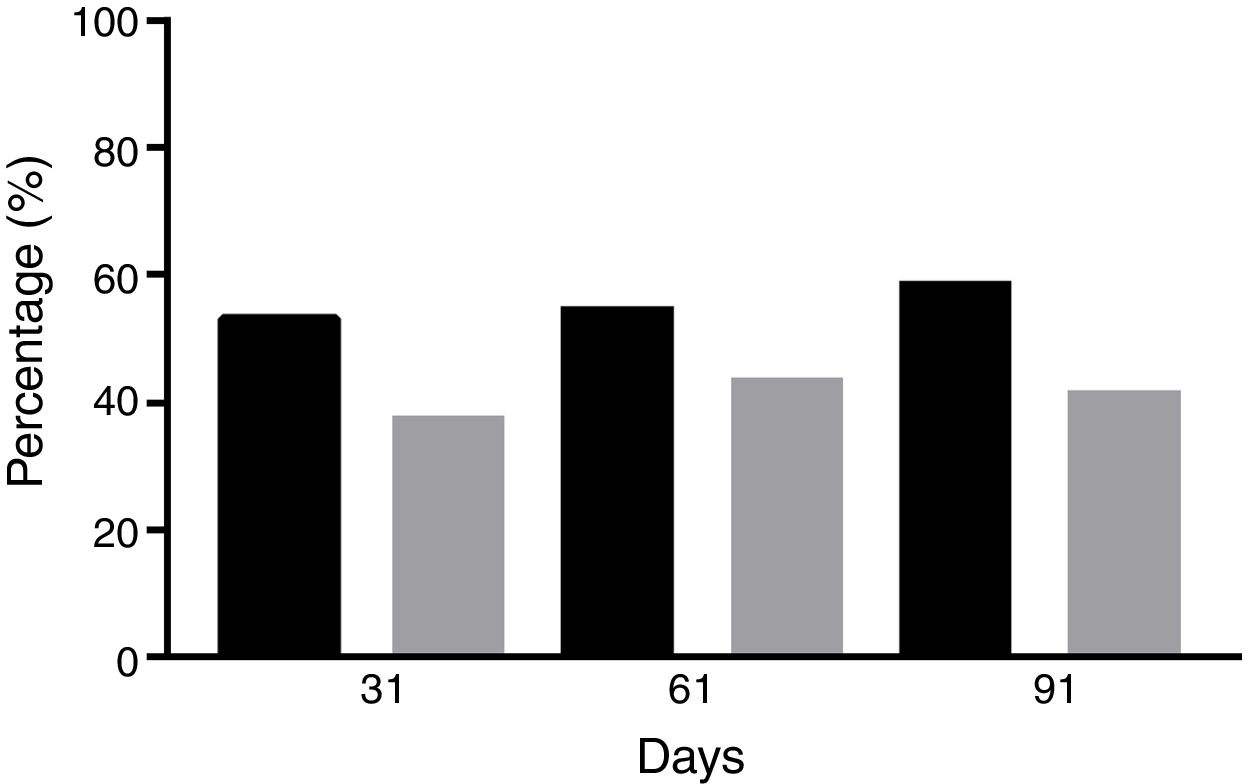
Forty-four male patients completed the study. The mean age was 28±12 years (range, 21–45 years), and the mean weight was 68.2±19.7kg (range 60–96kg). Sputum smear microscopy was negative in all patients after completion of the intensive phase and remained negative until completion of treatment. The mean dose of rifampicin administered was 9.37mg/kg/day (range 8.4–11.8mg/kg/day). At admission, there were no measurable concentrations of rifampicin in all blood samples. In the course of the treatment, the mean levels of rifampicin were 0.6μg/mL (95%CI=0.43–0.78μg/mL), 0.55μg/mL (95%CI=0.34–0.75μg/mL) and 0.46μg/mL (95%CI=0.32–0.60μg/mL) on days 31, 61 (phase 1) and 91 (phase 2), respectively (F=0.8409; p=0.4346) (Fig. 1). There was a 23% decrease in mean rifampicin levels in the course of treatment. Next, rifampicin levels were allocated as below or above the MIC. On days 31, 61 and 91, 52.2% (n=23), 54.5% (n=24), and 59% (n=26) of patients showed plasma levels of rifampicin below 0.5μg/mL (X2=0.192; p=0.9086), respectively (Fig. 2). Of those, 38% (n=17), 44% (n=19), and 42% (n=18) had concentrations of rifampicin below 0.25μg/mL (X2=0.111; p=0.946). The percentage of patients with conversion of sputum smears on day 31 was 70% (n=31), and 55% (n=17) had rifampicin plasma levels below 0.5μg/mL (X2=0.129; p=0.7194). On day 61, all patients showed conversion of sputum smears.

Time of exposure is more effective than the amount of absorbed drug to assess efficacy of rifampicin.3,8,12 In 70s, the ratio of pre-dose concentration to MIC was the most relevant pharmacodynamic index to assess rifampicin exposure.12 Thereafter, numerous ways to estimate exposure of M. tuberculosis to the drug were reported, such as the measurement of plasma concentration at 2h (Cmax) and 6h after drug administration or the ratio of 0–24h area under the concentration-time curve (AUC) to the minimum inhibitory concentration (AUC/MIC).3,8,13–15 However, there are limitations with both procedures, as collection of serial blood samples is a laborious and expensive process, and is generally not feasible in clinical practice.
In the study, the pre-dose samples were chosen to assess drug exposure based on the following assertions: (a) therapeutic doses should ensure effective plasma levels for 24h after rifampicin intake; and (b) the drug is active when blood concentrations are above the MIC.12,15 Furthermore, the sampling schedule was based on reports showing the ability of rifampicin to induce CYP isoforms is most evident in the early phase of the treatment.3,6,7,12
All plasma samples collected on D0 were negative for rifampicin, confirming that the drug had not been recently used by the patients enrolled in the study. The mean levels of rifampicin were above the MIC on days 31 and 61, but a high percentage of samples presented drug levels below 0.5μg/mL. This finding can be due to both the short half-life of the drug as well as to the normal variation of the residual levels of rifampicin.3,6,7,12
The concentrations of rifampicin were similar throughout the study, with a non-significant decrease of 23% in the course of the treatment, which could be due to the capacity of rifampicin to induce several CYP isoforms and transporters as MDR1 and MDR2. Such induction brings drug concentration to below the MIC and increases the range of residual levels of the drug.3,16,17 Furthermore, several factors related to the patients, to the drug, and to the policy of diagnosis and treatment of the disease also influence the concentrations of rifampicin.3,6,7,13,14 Therefore, rifampicin levels in pre-doses samples offer limited information on the exposure of M. tuberculosis.
The frequency of samples with drug levels below 0.5μg/mL was not associated with conversion of sputum microscopy, which corroborates the limited information of drug exposure in pre-doses samples as well as the difficulty to interpret clinical and bacteriological outcomes of a single drug in a four-drug regimen. Furthermore, variables of M. tuberculosis, as the various growth rates in vivo, make it difficult to correlate drug efficacy with time of concentration above the MIC.3,5,8,12
In conclusion, the levels of rifampicin were below the MIC in most of the samples in both phases of treatment, and there was no significant association between frequency of samples with drug levels below 0.5μg/mL with conversion of the sputum smears. These data suggest that pre-doses samples offer limited information on the exposure of M. tuberculosis to rifampicin.
FundingThere is no funding source to declare.
Conflicts of interestThe authors declare no conflicts of interest.
