
Several tools have been developed to evaluate HIV health-related quality of life (HRQoL) during and after antiretroviral therapy (ART). Few longitudinal studies evaluated the effect of ART on the quality of life of HIV patients.
ObjectiveTo evaluate changes in HRQoL in HIV-infected individuals one year after initiating ART.
MethodsA prospective study was conducted from May 2016 to July 2018. Data on clinical and sociodemographic characteristics of 91 HIV-infected patients were collected prior to initiation of ART and one year thereafter. Demographic and clinical data were collected and the questionnaires 36-item Short Form Health Survey (SF-36) and HIV/AIDS-targeted quality of life (HAT-QoL) were administered in both periods. Asymptomatic individuals, aged ≥18 years, were included in the study. Patients who discontinued treatment were excluded. The association between predictors of physical and mental HRQoL was analyzed by multiple linear regression analysis.
ResultsPatients were predominantly male (78.0%), mean age 35.3 ± 10.7 years, with no stable relationship (80.2%), and no comorbidities (73.6%). Most of the SF-36 domains improved after one year, particularly Physical Function (p = 0.0001), General Health (p = 0.0001), Social Functioning (p = 0.0001), Mental Health (p = 0.001), and Mental Component Summary (p = 0.004). HAT-QoL domains improved in the Overall Function (p = 0.0001), Life Satisfaction (p = 0.0001), Provider Trust (p = 0.001), and Sexual Function (p = 0.0001) domains. Sex (p = 0.032), age (p = 0.001), income (p = 0.007), and stable relationship (p = 0.004) were good predictors of the Physical Component Summary. Sex (p = 0.002) and stable relationship (p = 0.038) were good predictors of the Mental Component Summary. SF-36 and HAT-QoL scales presented strong correlations, except for Medication Concerns (0.15–0.37), HIV Mastery (0.18–0.38), Disclosure Worries (−0.15 to 0.07), and Provider Trust (−0.07 to 0.15).
ConclusionsART improved HRQoL after one year of use. The HAT-QoL and SF-36 correlated well and are good tools to evaluate HRQoL in HIV-infected patients on ART.
HIV infection has evolved from a deadly infection to a chronic disease in countries where treatment is widely available.1 Despite increase in life expectancy, health-related quality of life (HRQoL) of HIV patients is inferior than that observed in general population.2 Antiretroviral treatment programs had a significant impact on life expectancy in young populations, which resulted in a gain of approximately 14.4 million life-years between 1995 and 2009.3
HRQoL has a more restrict meaning, in comparison to the quality of life definition. It has been defined as the way health is estimated to affect individuals’ quality of life4 or the way a person perceives his/her well-being in physical, mental and social domains of health,5 as well as the way self-perceived well-being are related to or affected by the presence of disease or therapy. 6
Measuring HRQoL in patients on treatment allows the evaluation of medication benefits and side effects.7 However, there is no agreement in literature on the best approach for HRQoL measurement.8 Normative data for HRQoL generic instruments allows comparison with other groups, as well as the analysis of the influence of HIV and associated comorbidities on the HRQoL in a single evaluation.9
Several specific instruments to evaluate HIV-HRQoL have been developed, due to the assumption that specific HRQoL tools are superior when compared to generic instruments,8 as the HIV/AIDS-Targeted Quality of Life (HAT-QoL) scale.10 The use of specific instruments11 or the use of both, specific and generic, to evaluate HRQoL in HIV-inefected patients has been reported.12,13 Although the 36-Item Short Form Health Survey (SF-36)14 is a generic instrument, it has been preferred to evaluate HRQoL, rather than specific instruments, because of its lower ceiling and floor effect, good accuracy, and worldwide use.8,15
Questionnaires that use patient-reported outcomes may render valuable information about patient's health-related quality of life. Evaluating the effects of antiretroviral therapy in HRQOL of patients before and during ART is important for an integral patient approach. We aimed to evaluate the HRQoL in HIV-inefected individuals at baseline and after one year of ART.
Material and methodsA prospective cohort study was conducted from May 2016 to July 2018. Data on clinical and sociodemographic characteristics of HIV-infected patients were collected prior to the initiation of ART and one year thereafter. Patients who discontinued treatment were excluded. The sample was consecutive and non-probabilistic, and gathered at a Reference Outpatient Clinic of Infectious Diseases, in Salvador, Bahia, Brazil. All patients who agreed to participate in the study signed the informed consent form. The study included naïve and asymptomatic HIV-infected patients aged ≥18 years. HIV pregnant women, patients with active opportunistic infections or those who already on antiretroviral therapy were excluded. The study was approved by the institutional Ethics and Research Committee, protocol number 1,393,890.
To evaluate health-related quality of life, two questionnaires were used: the 36-item Short Form Health Survey (SF-36)14,15 and the HIV/AIDS Targeted Quality of Life (HAT-QoL).15 Both questionnaires were administered before initiation of ART and after one year of treatment.
The SF-36 has 36 items and evaluates health-related quality of life in eight domains: physical functioning (PF), role limitations due to physical problems (RF), bodily pain (BP), general health perceptions (GH), vitality (VT), social functioning (SF), role limitations due to emotional problems (RE), and mental health (MH). The eight scales were aggregated into a physical component summary (PCS) and a mental component summary (MCS) scores. SF-36 scores range from 0 to 100, where higher scores represent better HRQoL.14 Scores were normalized, using the Optum ProCore program version 1.0.6431.17600. Normalization was based on norms with a mean of 50 and a standard deviation of 10.14 Outcomes should be interpreted as below or above the US general population T score. All the normalized SF-36 scores have the same variance and can be compared with each other. This study was licensed by OptumInsight Life Sciences Inc, number QM025905.
The (HATQoL) instrument is a 34-item HIV specific health-related quality of life questionnaire. The instrument assesses nine domains, including overall function, life satisfaction, health worries, financial worries, medication worries, HIV mastery, disclosure worries, provider trust, and sexual function. The nine domains are transformed to a linear 0–100 scale where 0 is the worst possible outcome and 100 the best possible outcome.10
The Charlson comorbidity index (CCI) was used to access severity of comorbid diseases classified as mild (CCI scores of 1–2), moderate (CCI scores of 3–4), and severe (CCI scores ≥5). 16
Cronbach’s Alpha coefficient was used to assess internal consistency, considering values under 0.60 to 0.70 as satisfactory17 and higher than 0.70 as ideal.18 Pearson correlation coefficient was used to analyze linear relationships between the instruments domains, considering results from 0.50 to 0.70 as moderate correlation, and 0.70 to 0.90 as high correlation.19
Data were analyzed using the Statistical Package for Social Sciences (SPSS) version 21. We used descriptive statistics, means and standard deviations for continuous variables, and percentages for categorical variables. Student's t-test for paired samples was used to compare the differences between the groups before and after ART and chi-square test to compare proportions between dependent and independent samples. The association between predictive variables and physical and mental HRQoL was analyzed by using multiple linear regression analysis. Variables (age, sex, education, family income, marital status, living with family, Charlson’s comorbidity index, body mass index [BMI], CD4 and CD8 counts, and HIV viral load) were selected according to univariate analysis. Variables with p-value ≤0.2520 were included in the multivariate analysis.
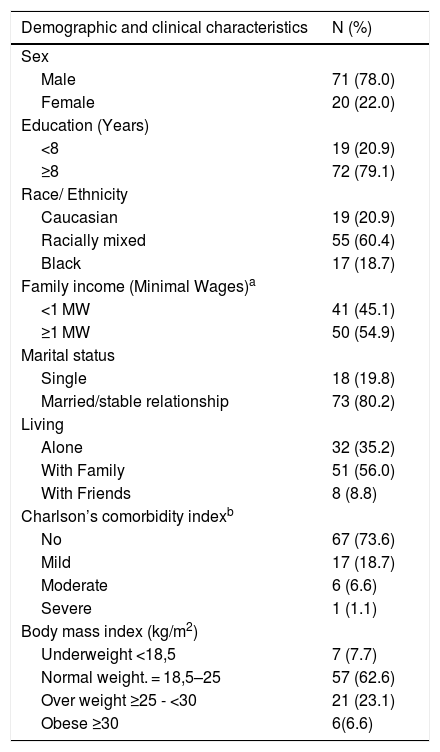
ResultsThe sample consisted of 91 HIV-infected patients, mean age 35.3 ± 10.7 years, evaluated at baseline and after one year of ART. Patients did not change therapy during the period of study. In the baseline evaluation, the means of CD4+ and CD8+ count were 407.2 ± 261.4 cell/mm3 and 1270.7 ± 727.1 cells/mm3. In addition, all patients presented detectable viral load (median viral load 4.60 log10 copies/ml IQR: 0.05–5.13). The majority were male (78.0%), racially mixed (60.4%), without stable relationship (80.2%), with equal or more than eight years of schooling (79.1%), living with family (56.0%), no comorbidities (73.6%), and with normal BMI (62.6%) (Table 1). BMI slightly increased after one year of ART (from 23.3 ± 4.1 kg/m² to 24.9 ± 4.3 kg/m²).
Demographic and clinical characteristics of the 91 HIV-infected patients. Salvador, Bahia, Brazil, 2018.
| Demographic and clinical characteristics | N (%) |
|---|---|
| Sex | |
| Male | 71 (78.0) |
| Female | 20 (22.0) |
| Education (Years) | |
| <8 | 19 (20.9) |
| ≥8 | 72 (79.1) |
| Race/ Ethnicity | |
| Caucasian | 19 (20.9) |
| Racially mixed | 55 (60.4) |
| Black | 17 (18.7) |
| Family income (Minimal Wages)a | |
| <1 MW | 41 (45.1) |
| ≥1 MW | 50 (54.9) |
| Marital status | |
| Single | 18 (19.8) |
| Married/stable relationship | 73 (80.2) |
| Living | |
| Alone | 32 (35.2) |
| With Family | 51 (56.0) |
| With Friends | 8 (8.8) |
| Charlson’s comorbidity indexb | |
| No | 67 (73.6) |
| Mild | 17 (18.7) |
| Moderate | 6 (6.6) |
| Severe | 1 (1.1) |
| Body mass index (kg/m2) | |
| Underweight <18,5 | 7 (7.7) |
| Normal weight. = 18,5–25 | 57 (62.6) |
| Over weight ≥25 - <30 | 21 (23.1) |
| Obese ≥30 | 6(6.6) |
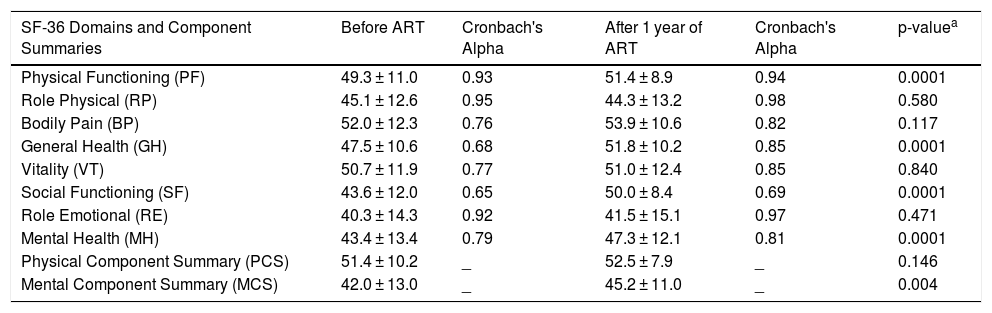
Both health-related quality of life instruments presented reliability above the desirable Cronbach's Alpha (≥0.6) for all domains. Table 2 showed the description of the HRQoL according to the SF-36 scores. The SF-36 scores were systematically higher after one year of ART, except for the Role Physical domain (p = 0.580). Physical Functioning (p = 0.0001), General health (p = 0.0001), Social Functioning p = 0.0001), Mental Health (p = 0.0001), and Mental Component Summary (p = 0.004) were significantly higher after one year of ART.
Means and standard deviations of SF-36 Health-Related Quality of Life normalized scores in 91 HIV-infected patients at baseline and after one year of ART. Salvador, Bahia, Brazil, 2018.
| SF-36 Domains and Component Summaries | Before ART | Cronbach's Alpha | After 1 year of ART | Cronbach's Alpha | p-valuea |
|---|---|---|---|---|---|
| Physical Functioning (PF) | 49.3 ± 11.0 | 0.93 | 51.4 ± 8.9 | 0.94 | 0.0001 |
| Role Physical (RP) | 45.1 ± 12.6 | 0.95 | 44.3 ± 13.2 | 0.98 | 0.580 |
| Bodily Pain (BP) | 52.0 ± 12.3 | 0.76 | 53.9 ± 10.6 | 0.82 | 0.117 |
| General Health (GH) | 47.5 ± 10.6 | 0.68 | 51.8 ± 10.2 | 0.85 | 0.0001 |
| Vitality (VT) | 50.7 ± 11.9 | 0.77 | 51.0 ± 12.4 | 0.85 | 0.840 |
| Social Functioning (SF) | 43.6 ± 12.0 | 0.65 | 50.0 ± 8.4 | 0.69 | 0.0001 |
| Role Emotional (RE) | 40.3 ± 14.3 | 0.92 | 41.5 ± 15.1 | 0.97 | 0.471 |
| Mental Health (MH) | 43.4 ± 13.4 | 0.79 | 47.3 ± 12.1 | 0.81 | 0.0001 |
| Physical Component Summary (PCS) | 51.4 ± 10.2 | _ | 52.5 ± 7.9 | _ | 0.146 |
| Mental Component Summary (MCS) | 42.0 ± 13.0 | _ | 45.2 ± 11.0 | _ | 0.004 |
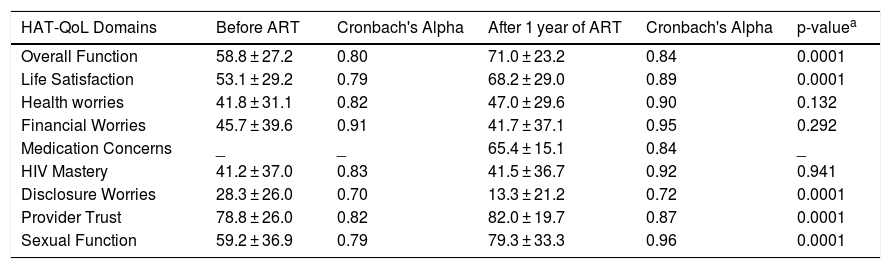
After one year of ART, the scores of the HAT-QoL domains Overall Funcion (p = 0.0001), Life Satisfaction (p = 0.0001), Provider Trust (p = 0.001) and Sexual Function (p = 0.0001) were significantly higher, and Disclosure Worries was significantly lower (p = 0.0001). Health Worries and HIV Mastery domains were also slightly higher, but the differences did not reach statistical significance. Financial worries showed a slight decrease (p = 0.292) after one year of treatment. (Table 3).
Means and standard deviations of HAT-QoL in 91 HIV patients, before and after one year of ART. Salvador, Bahia, Brazil, 2018.
| HAT-QoL Domains | Before ART | Cronbach's Alpha | After 1 year of ART | Cronbach's Alpha | p-valuea |
|---|---|---|---|---|---|
| Overall Function | 58.8 ± 27.2 | 0.80 | 71.0 ± 23.2 | 0.84 | 0.0001 |
| Life Satisfaction | 53.1 ± 29.2 | 0.79 | 68.2 ± 29.0 | 0.89 | 0.0001 |
| Health worries | 41.8 ± 31.1 | 0.82 | 47.0 ± 29.6 | 0.90 | 0.132 |
| Financial Worries | 45.7 ± 39.6 | 0.91 | 41.7 ± 37.1 | 0.95 | 0.292 |
| Medication Concerns | _ | _ | 65.4 ± 15.1 | 0.84 | _ |
| HIV Mastery | 41.2 ± 37.0 | 0.83 | 41.5 ± 36.7 | 0.92 | 0.941 |
| Disclosure Worries | 28.3 ± 26.0 | 0.70 | 13.3 ± 21.2 | 0.72 | 0.0001 |
| Provider Trust | 78.8 ± 26.0 | 0.82 | 82.0 ± 19.7 | 0.87 | 0.0001 |
| Sexual Function | 59.2 ± 36.9 | 0.79 | 79.3 ± 33.3 | 0.96 | 0.0001 |
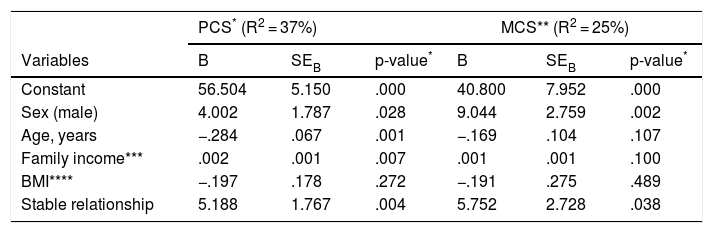
The association of predictor variables with the SF-36 physical and mental components was explored using multivariate linear regression analysis (Table 4). Sex (p = 0.028), age (p = 0.001), income (p = 0.007), and stable relationship (p = 0.004) were predictors for physical component summary. Male sex (p = 0.002) and stable relationship (p = 0.038) were predictors of the mental component summary.
Results of a multiple linear regression equation having PCS and MCS as the dependent variable for 91 HIV- patients. Salvador, Bahia, Brazil, 2018.
| PCS* (R2 = 37%) | MCS** (R2 = 25%) | ||||||
|---|---|---|---|---|---|---|---|
| Variables | B | SEB | p-value* | B | SEB | p-value* | |
| Constant | 56.504 | 5.150 | .000 | 40.800 | 7.952 | .000 | |
| Sex (male) | 4.002 | 1.787 | .028 | 9.044 | 2.759 | .002 | |
| Age, years | −.284 | .067 | .001 | −.169 | .104 | .107 | |
| Family income*** | .002 | .001 | .007 | .001 | .001 | .100 | |
| BMI**** | −.197 | .178 | .272 | −.191 | .275 | .489 | |
| Stable relationship | 5.188 | 1.767 | .004 | 5.752 | 2.728 | .038 | |
The numbers in columns are regression coefficients (B), standard errors (SEB) and P values.
*PCS- Physical Component Summary; ** Mental Component Summary; ***Family income (Minimal Wages): MW: USD 285.00; ****BMI- Body Mass Index (kg/m2).
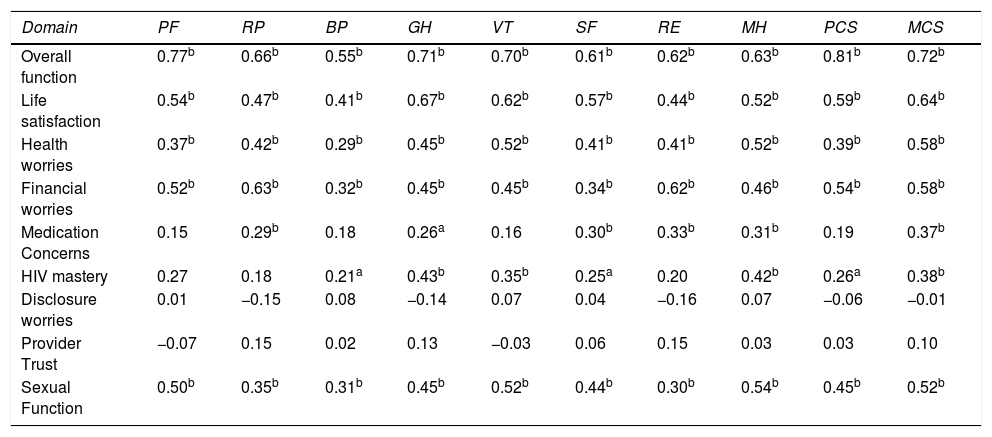
SF-36 and HAT-QoL domains were strongly correlated, except for Medication Concerns (0.15–0.37), HIV Mastery (0.18 to 0.38), Disclosure Worries (-0.15 to 0.07) and Provider Trust (-0.07 to 0.15) domains. The HATQoL domain Overall function presented the highest correlation with SF-36 domains, all being above 0.60, except for BP (0.55) as shown in Table 5.
Pearson correlation among SF-36 and HAT-QoL domains in 91 HIV-infected patients after one year of ART. Salvador, Bahia, Brazil, 2018.
| Domain | PF | RP | BP | GH | VT | SF | RE | MH | PCS | MCS |
|---|---|---|---|---|---|---|---|---|---|---|
| Overall function | 0.77b | 0.66b | 0.55b | 0.71b | 0.70b | 0.61b | 0.62b | 0.63b | 0.81b | 0.72b |
| Life satisfaction | 0.54b | 0.47b | 0.41b | 0.67b | 0.62b | 0.57b | 0.44b | 0.52b | 0.59b | 0.64b |
| Health worries | 0.37b | 0.42b | 0.29b | 0.45b | 0.52b | 0.41b | 0.41b | 0.52b | 0.39b | 0.58b |
| Financial worries | 0.52b | 0.63b | 0.32b | 0.45b | 0.45b | 0.34b | 0.62b | 0.46b | 0.54b | 0.58b |
| Medication Concerns | 0.15 | 0.29b | 0.18 | 0.26a | 0.16 | 0.30b | 0.33b | 0.31b | 0.19 | 0.37b |
| HIV mastery | 0.27 | 0.18 | 0.21a | 0.43b | 0.35b | 0.25a | 0.20 | 0.42b | 0.26a | 0.38b |
| Disclosure worries | 0.01 | −0.15 | 0.08 | −0.14 | 0.07 | 0.04 | −0.16 | 0.07 | −0.06 | −0.01 |
| Provider Trust | −0.07 | 0.15 | 0.02 | 0.13 | −0.03 | 0.06 | 0.15 | 0.03 | 0.03 | 0.10 |
| Sexual Function | 0.50b | 0.35b | 0.31b | 0.45b | 0.52b | 0.44b | 0.30b | 0.54b | 0.45b | 0.52b |
Our prospective study showed an improvement in the HRQOL of HIV-infected individuals after one year of ART, using SF-36 and HAT-QoL. We demonstrated that SF-36 and HATQoL presented good correlations for most domains, except for Medication Concerns, HIV Mastery, Disclosure Worries, and Provider Trust. The highest HAT-QoL correlation with SF-36 occurred in the Overall Function domain (0.61-0.81). The HAT-QoL scale measures different aspects, which reinforces the use of both a specific and a general instruments, to better measuring HRQOL in individuals living with HIV/AIDS.12 Both instruments presented good internal consistence in all domains, considering Cronbach’s Alpha coefficient values from 0.60 to 0.70, as satisfactory17 and higher than 0.70 as ideal.18 However, there is no consensus on literature about interpretation of these correlations.
Despite the low frequency of patients with comorbidities, the instruments were able to identify improvements in their health-related quality of life, considering physical and mental aspects. After one year of ART significant improvements were observed in Physical Functioning, General Health, Social Functioning, Mental Health, and Mental Component Summary. The use of normalized SF-36 scores showed that all patients were stable and had scores of HRQoL instrument at baseline close to the expected value (50 ± 10). All SF-36 domains were higher after one year of ART, except for the Role Physical domain, which presented a non-significant slight decrease (p = 0.58). However, the result was not below the expected value.
The recent diagnosis at study entry may have induced a worst perception of patients about their HRQoL,21 which may justify the improvement of SF-36 domains. In contrast, HIV infection itself may have a negative impact on patients' physical and mental HRQOL,22 even after the initiation of ART, compared to the general population.2 In addition, HIV infection is a chronic disease that may decrease patients’ physical health,23,24 including the mental aspects of health.
The impact of antiretroviral therapy in HIV-infected patients, is still controversial. The worsening of motor function and health-related quality of life in HIV-patients have been reported,25 while physical functioning26 and HRQoL27 of asymptomatic infected individuals have been reported to be similar to that of the general population or non-infected healthy individuals.
Although our results show an increase of 6.5% in mean BMI after one year of ART, this index was not a predictor of HRQoL in the linear multivariate regression analysis. Nevertheless, metabolic and body fat changes during ART should be monitored28 with caution, as these effects may negatively impact the HRQoL of these patients.
Being male, young, with with a stable relationship, and with higher income were good predictors of the SF-36 Physical Component Summary by linear multivariate analysis. The association of higher PCS with male sex has been previously reported.29,30 Being female was predictive of lower MCS, while having a stable relationship was a predictor of higher MCS and PCS. These findings are in line with previous studies, that associated lower mental health scores to younger age, female sex, living alone, and fewer years of schooling,22 and physical impairment.30,31,32 However, a Chinese cohort showed no differences in the HRQoL scores by sex during the first six months after starting ART.33 The same study also revealed higher HRQoL scores associated with stable relationship,33 while another study associated the variable with lower Physical functioning. 29
Significant improvement in MCS after one year of ART is consistent with previous studies. Despite the likelihood of ART adverse effects on physical well-being, early introduction of ART significantly increases psychological well-being over the years, and decreases morbidity.21 Patients’ understanding of HIV-infection, as well as the benefits of controlling infections with ART, leads to less anxiety in HIV-infected patients.21,34 Depression is the most frequent psychiatric disorder in HIV-infected patients and is related with severity of symptoms35 and patients’ negative self-image.36 Interruption of ART and low social support also contributed for decreasing of MCS in infected patients.37
The absence of normalized data may difficult HAT-QoL interpretation in cross-sectional studies. However, using HAT-QoL together with a normalized instrument or in longitudinal studies allow for comparisons at different times and may add specific patient outcome that is not measured with a HRQoL general instrument. In our study, the HAT-QoL questionnaire was also capable of detecting differences in asymptomatic patients before and after one year of treatment. The mean of HAT-QoL scores presented large standard deviation associated with wide distribution of scores. Our sample presented significant improvement in Overall Function, Life Satisfaction, Provider Trust and Sexual Function HAT-QoL domains. Such results may be explained by the positive impact of ART, improving patients’ general health, satisfaction with life and perspectives for life. 38
The HAT-QoL domain Disclosure Worries significantly decreased while Provider Trust significantly increased after one year of ART, evidencing that despite of good physician-patient relationship, HIV-infected patients need specialized psychological care to improve health-related quality of life. The fear of stigma and discrimination by infected patients is related to a greater concern with secrecy, decreasing patients’ HRQoL. 31
The improvement in HAT-QoL Sexual Function domain after one year of ART corroborated the improvement of Physical Functioning, General Health, Social Functioning, and Mental Health measured by SF-36. The correlation of HAT-QoL Sexual Function domain with SF-36 was good in both mental and physical domains. The affective-sexual relationship represents an important aspect for HRQoL in HIV-infected patients. The partner is important for emotional support, which is directly associated with better HRQoL.39 Our results underscore that stable relationship was good predictor of both mental (MCS) and physical (PCS) SF-36 summaries.
The simultaneous use of instruments with specific and generic dimensions, brought benefits to this study, since it expanded the dimension of the specific information about the HRQoL of individuals. While HAT-QoL is considered a specific instrument for the seropositive population, the SF-36 has satisfactory internal consistence and normative data, allowing clinical interpretation of HRQoL even in cross-sectional studies with good precision. A recent study also evidenced the benefits of using multiple instruments when accessing HIV outcomes. Authors investigated physical and psychological themes associated to HIV by using different validated instruments. Social support, self-esteem, and sexual difficulties were associated with general health.40
Our study has some limitations such as the impossibility of random allocation of participants. In addition, different ART regimens and health care providers could be important factors in determining changes in HRQoL for HIV patients. However, the initial ART regimen is standardized in Brazil, which means all patients receive the same regimen. In addition, the AIDS clinic are attended by the same health professionals, and initial cases are usually discussed with the Clinic Coordinator, which guarantees a similar standard of care for all patients. We conducted our study at a single State reference center for HIV, which could introduce some bias. However, it is the second largest HIV referral center in the state, and its population reflects the overall characteristics of HIV-infected patients in Bahia. Longitudinal studies allow for more precise evaluation, establishing cause and effect. Measures of patient-reported outcomes of quality of life are necessarily subjective, and this can make the study vulnerable to recall bias. To reduce this effect, the researchers used two quality of life instruments, both with good reliability.
In conclusion, ART improved HRQoL of HIV-infected patients after one year of treatment. The SF-36 and HATQoL showed good correlations, mainly in Overall Function Domain and presented good internal consistence in all domains. We recommend the use of both specific and general instruments for measuring HRQoL in HIV-infected patients. Having a stable relationship was a good predictor of better mental (PCS) and physical (MCS) health. Male sex, being young, and having higher income were good predictors of the physical health component, while being female was predictor of lower mental health (MCS).
Conflict of interestThe authors declare no conflict of interest.
