
Interferon-α based therapy for chronic hepatitis C (CHC) is associated with thyroiditis and thyroid dysfunction (TD). This study investigated whether TD during pegylated interferon-α (PEG-IFN) plus ribavirin treatment favors sustained viral response (SVR), and also the association between TD and PEG-IFN formulations. This retrospective study was performed in CHC patients who had received PEG-IFN plus ribavirin and had been followed for six months after treatment. Several factors were compared between patients with and without TD. 119 patients were included in the study. De novo incidence of TD was found to be 16.8%, and 16 of the 18 patients with TD achieved SVR. Although this rate was higher than patients without TD according to univariate analysis, logistic regression analysis revealed that there was not a significant association between TD and SVR, whereas baseline thyroperoxidase antibody (anti-TPO) positivity was the only significant predictor of TD. Moreover, TD was not associated with PEG-IFN type. Both interferon-α and hepatitis C virus (HCV) contribute to TD during antiviral therapy. It seems that there is no association between thyroid toxicity and viral clearance or type of PEG-IFN; however, anti-TPO positivity before treatment is the strongest predictor for TD during antiviral therapy.
Pegylated interferon (PEG-IFN) plus ribavirin is the current standard of care for the treatment of chronic hepatitis C (CHC).1 This treatment regimen has several adverse effects, including autoimmune disorders. Thyroid dysfunction (TD) represents the most common autoimmune disorder observed during CHC treatment.2 The incidence of TD during interferon-α (IFN-α) plus ribavirin combination therapy has been reported to occur in 4.7% to 27.8% of patients, with a mean incidence of 12.1%.3 This condition may be the result of immune activation by interferon.
While the epidemiology and clinical presentation of IFN-induced TD in CHC patients have been well characterized, the mechanisms causing this condition are still poorly understood. Also, there are few studies that assess the relationship between TD and viral kinetics or virological outcome, as well as the effects of the pegylated form of IFN-α on the thyroid gland.3,4 This study investigated whether TD during PEG-IFN plus ribavirin treatment of CHC is associated with treatment formulations (PEG-IFNα-2a or 2b) or sustained viral response (SVR), and also aimed to find the significant predictors for TD.
Materials and methodsPatients who received treatment for CHC at the infectious diseases clinic of Gaziosmanpasa university hospital in Tokat, Turkey between the years 2005 and 2010 were included in the study. Eligible subjects were: CHC patients who had received weekly injections of PEG-IFNα-2a or -2b plus ribavirin orally for 48 weeks, followed for 24 weeks after treatment, who had normal pretreatment TSH levels, and had been examined serially for thyroid functions as well as other required parameters (thyroid abnormalities were monitored at monthly intervals). PEG-IFNα-2a was administered once a week at a daily dose of 180μg, and PEG-IFNα-2b was administered once a week at a daily dose of 1.5μg/kg of body weight. Ribavirin was orally administered daily in two divided doses (1,000mg for ≤ 75kg, 1,200mg for > 75 kg).
Patients with hepatitis B virus infection, HIV infection, autoimmune hepatitis, primary biliary cirrhosis, alcoholic liver disease, or Wilson's disease were excluded. Patients were classified as responders if they achieved SVR, defined as undetectable hepatitis C virus (HCV)-RNA at six months after completion of antiviral therapy. The remaining patients were categorized as non-SVR. Patients with TD were received appropriate therapy for hypo- or hyperthyroidism during the course of antiviral therapy. HCV genotyping was performed only for patients admitted after September 2009.
Statistical analysisAccording to Kolmogorov-Smimov normality test, the t-test for two independent samples was used to compare age and Knodell score between two groups. Continuous data were expressed as mean ± standard deviation (SD). The chi-squared test was used for comparing categorical data. Categorical data were expressed as count (n) and percentages (%). A multiple logistic regression model was implemented to determine the risk factors independently associated with TD. p-values below 0.05 were considered statistically significant. Statistical analysis was performed by using the Statistical Package for Social Sciences software (SPSS Statistics 19, SPSS inc., an IBM Co. – Somers, NY)
Ethics statementThe study protocol was approved by the institutional review board of the Gaziosmanpasa University, Tokat, Turkey (IRB No. 12BADK021).
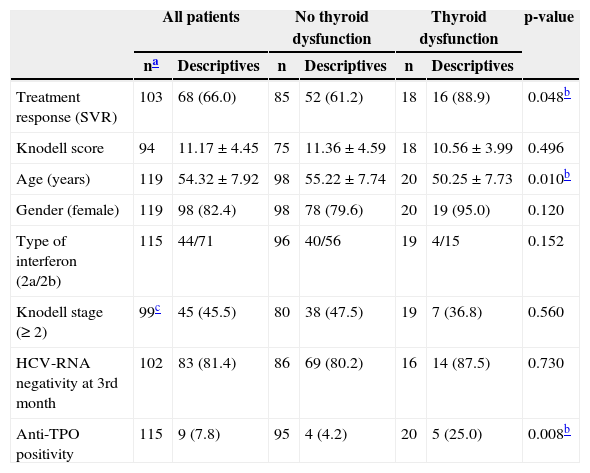
ResultsA total of 119 CHC patients who had completed the course of antiviral treatment in the period of 2005 to 2010 were eligible for the study. Two patients discontinued treatment at the third month due to severe side effects; two other patients stopped therapy as they failed to drop quantitative HCV-RNA in at least 2 log at the third month (early virological nonresponder). These two patients were regarded as nonresponders, as well as those who still had detectable HCV-RNA at the sixth month. The remaining patients received at least six months of therapy. The non-SVR group comprised nonresponders and relapsers. The mean age of the 119 patients was 54.32 years, consisting of 98 women and 21 men. 20 of the 119 patients (16.8%) developed TD during therapy. 12 patients had hyperthyroidism and eight had hypothyroidism by abnormal thyroid function tests, firstly determined during therapy. When the parameters between TD patients and euthyroid patients were compared, the univariate analysis revealed that the presence of anti-thyroperoxidase (anti-TPO) antibodies before treatment was more common in patients with TD than without TD, and patients in the TD group were younger than patients in the other group (p = 0.008, p = 0.01). When evaluating liver fibrosis of the two groups according to Knodell staging, the number of patients having liver fibrosis of Knodell stage > 1 was comparable between the two groups (Table 1). Of 119 patients, 16 patients did not have the data for SVR because of early discontinuation of therapy due to a side effect or insufficient time elapsed after completion of therapy. Of 103 patients, 68 (66%) achieved SVR. According to the univariate analysis, TD patients achieved SVR more frequently than euthyroid patients (p = 0.048), although there was not a significant difference between the groups regarding HCV-RNA negativity at third month of therapy. Analysis also showed that TD was not associated with PEG-IFN formulations. The findings of the univariate analysis are summarized in Table 1.
Characteristics of CHC patients including those with and without thyroid dysfunction.
| All patients | No thyroid dysfunction | Thyroid dysfunction | p-value | ||||
|---|---|---|---|---|---|---|---|
| na | Descriptives | n | Descriptives | n | Descriptives | ||
| Treatment response (SVR) | 103 | 68 (66.0) | 85 | 52 (61.2) | 18 | 16 (88.9) | 0.048b |
| Knodell score | 94 | 11.17 ± 4.45 | 75 | 11.36 ± 4.59 | 18 | 10.56 ± 3.99 | 0.496 |
| Age (years) | 119 | 54.32 ± 7.92 | 98 | 55.22 ± 7.74 | 20 | 50.25 ± 7.73 | 0.010b |
| Gender (female) | 119 | 98 (82.4) | 98 | 78 (79.6) | 20 | 19 (95.0) | 0.120 |
| Type of interferon (2a/2b) | 115 | 44/71 | 96 | 40/56 | 19 | 4/15 | 0.152 |
| Knodell stage (≥ 2) | 99c | 45 (45.5) | 80 | 38 (47.5) | 19 | 7 (36.8) | 0.560 |
| HCV-RNA negativity at 3rd month | 102 | 83 (81.4) | 86 | 69 (80.2) | 16 | 14 (87.5) | 0.730 |
| Anti-TPO positivity | 115 | 9 (7.8) | 95 | 4 (4.2) | 20 | 5 (25.0) | 0.008b |
SVR, sustained viral response; TPO, thyroperoxidase.
HCV genotyping was performed in only 26 patients, and all were found to have genotype 1. Due to this finding and to the fact that the majority of Turkish HCV patients have genotype 1, statistical analysis regarding the genotype was not included in this study.5
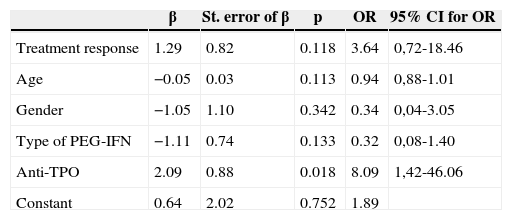
Multiple logistic regression analysis was performed to determine the independent factors related to TD among parameters that might affect TD, including age, gender, treatment response, PEG-IFN formulations, and anti-TPO, and it was found that anti-TPO was the only risk factor for TD (Table 2).
Multiple logistic regression analysis of factors associated with TD.
| β | St. error of β | p | OR | 95% CI for OR | |
|---|---|---|---|---|---|
| Treatment response | 1.29 | 0.82 | 0.118 | 3.64 | 0,72-18.46 |
| Age | −0.05 | 0.03 | 0.113 | 0.94 | 0,88-1.01 |
| Gender | −1.05 | 1.10 | 0.342 | 0.34 | 0,04-3.05 |
| Type of PEG-IFN | −1.11 | 0.74 | 0.133 | 0.32 | 0,08-1.40 |
| Anti-TPO | 2.09 | 0.88 | 0.018 | 8.09 | 1,42-46.06 |
| Constant | 0.64 | 2.02 | 0.752 | 1.89 |
TD, thyroid dysfunction; OR, odds ratio; PEG-INF, pegylated interferon-α; TPO, thyroperoxidase.
PEG-IFN and ribavirin combination therapy is the current standard treatment for CHC. This treatment regimen provides a cure rate of approximately 50%. Patients with HCV genotype 2 or 3 have a better response to treatment than genotype 1 patients.1 Other favorable factors in response to treatment include viral load (patients with low viral load have a better response), younger age, female gender, mild liver fibrosis, compliance, duration of treatment, early viral load reduction, and low body mass index.6,7 However, there is controversy in the literature regarding the relationship between TD and SVR. In this study, TD was not associated with SVR after logistic regression analysis, although SVR was more commonly achieved in patients with TD, according to the univariate analysis. In a study published in 2002, Dalgard et al. showed that TD induced by standard IFN-α therapy had no correlation with SVR rate.8 In a recent study by Tran et al.,4 the authors reported a positive and significant association between thyroid disease and viral clearance. However, in another study published in the same year, Vezali et al.9 investigated possible prognostic factors for TD development, including pretreatment virological parameters and viral kinetics or virological outcome, and concluded that TD did not appear to be linked to viral kinetics or SVR.
Chronic HCV infection has been shown to be associated with thyroid autoimmunity and TD.3,10 Moreover, thyroid disease may also be a side effect of IFN-based treatment.2 According to previous studies, approximately 12% of patients (ranging from 4.7% to 27.8%) receiving IFN-α and ribavirin combination therapy will develop TD.3,9 Although many studies have focused mostly on combination therapy with IFN-α plus ribavirin, there are few data regarding the effect of PEG-IFN. Jamil et al. reported that patients who used PEG-IFN had higher risk of TD than those using conventional interferon (14% vs. 7%, p = 0.038).11 However, in contrast to this finding, Tran et al.12 found that the pegylation of IFN, in combination with ribavirin, did not cause more thyroid diseases than the classic IFN plus ribavirin in the hepatitis C population, as the result of a meta-analysis. In a previous report, the authors found that the incidence of TD in CHC patients receiving PEG-IFN plus ribavirin therapy was 11.4%, while in the current study the incidence was found to be a little higher, however, both were consistent with the literature.13
The most common manifestation of IFN-induced thyroid disease has been reported to be autoimmune thyroiditis, predominantly Hashimoto's thyroiditis. Other autoimmune thyroid abnormalities include Graves’ disease or increased serum anti-thyroid antibody concentrations without TD. Also, recent data suggest that, in addition to its immunomodulatory mechanism, IFN-α also precipitates thyroiditis by direct thyrotoxic effects.14–16 The main risk factor for developing thyroid disease in the course of antiviral therapy is previous positivity for anti-thyroid antibodies, especially in older women.3,15,17 In the present study, after univariate analysis, the mean age of patients with TD was lower than that of patients without TD (50 versus 55), and SVR and pretreatment anti-TPO were more commonly found in the TD group, while TD was not found to be associated with gender, liver histology, PEG-IFN formulation, or HCV-RNA negativity at the third month. However, among the parameters mentioned above, only anti-TPO positivity was found to be an independent risk factor for TD as a result of multivariate analysis. An interesting finding of this study was that TD showed no association with virologic response, as well as no association to PEG-IFN formulations. The present findings were compatible with the findings in the study by Vezali et al.,9 where they reported that early virologic response, SVR, and PEG-IFN formulations were not risk factors for TD, but were linked to development of other therapy-related autoimmune disorders. Vezali et al. also found that HCV genotyping was not associated with TD.
A limitation of this study was that baseline HCV viral load could not be compared between the patients with TD and without TD because different quantitative HCV-RNA assays were applied to patients over a period of five years. Because this patient population consisted of patients coming from a single region of Anatolia, forming a homogenous population in terms of HCV genotype (predominantly genotype 1), multicentric studies are needed to show the association between genotype and TD.
In conclusion, it is suggested that TD can be predicted by pretreatment anti-TPO positivity while it seems not to be associated with the PEG-IFN-α formulations, early virologic response, or virological outcome in treated patients. Further prospective studies are needed to confirm these findings and to clarify the role of CHC per se in TD. Finally, CHC patients should be screened by thyroid function tests before and during antiviral therapy.
Conflicts of interestAll authors declare to have no conflict of interest.
