
Fluorodeoxyglucose positron emission tomography/computed tomography (PET/CT) is a powerful tool in cancer imaging. The basic principle is the accumulation of the radiopharmaceutical in areas of increased glucose metabolism. However, glucose is also an important substrate for inflammatory cells. Recent studies suggested that PET/CT findings should be interpreted with caution in tuberculosis-endemic regions.1,2 Here we reported the images of two cases with pulmonary tuberculosis mimicking lung cancer.
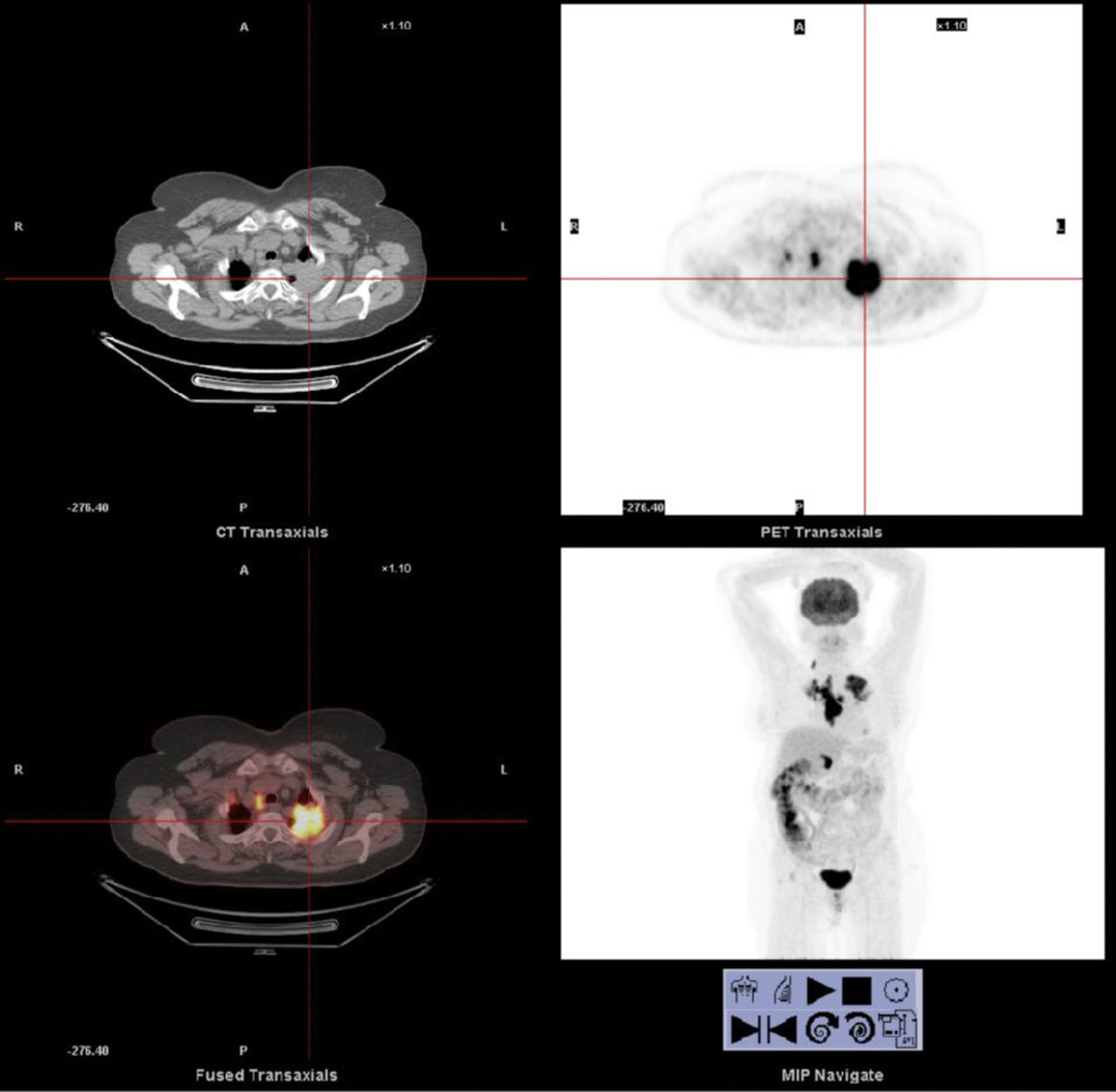
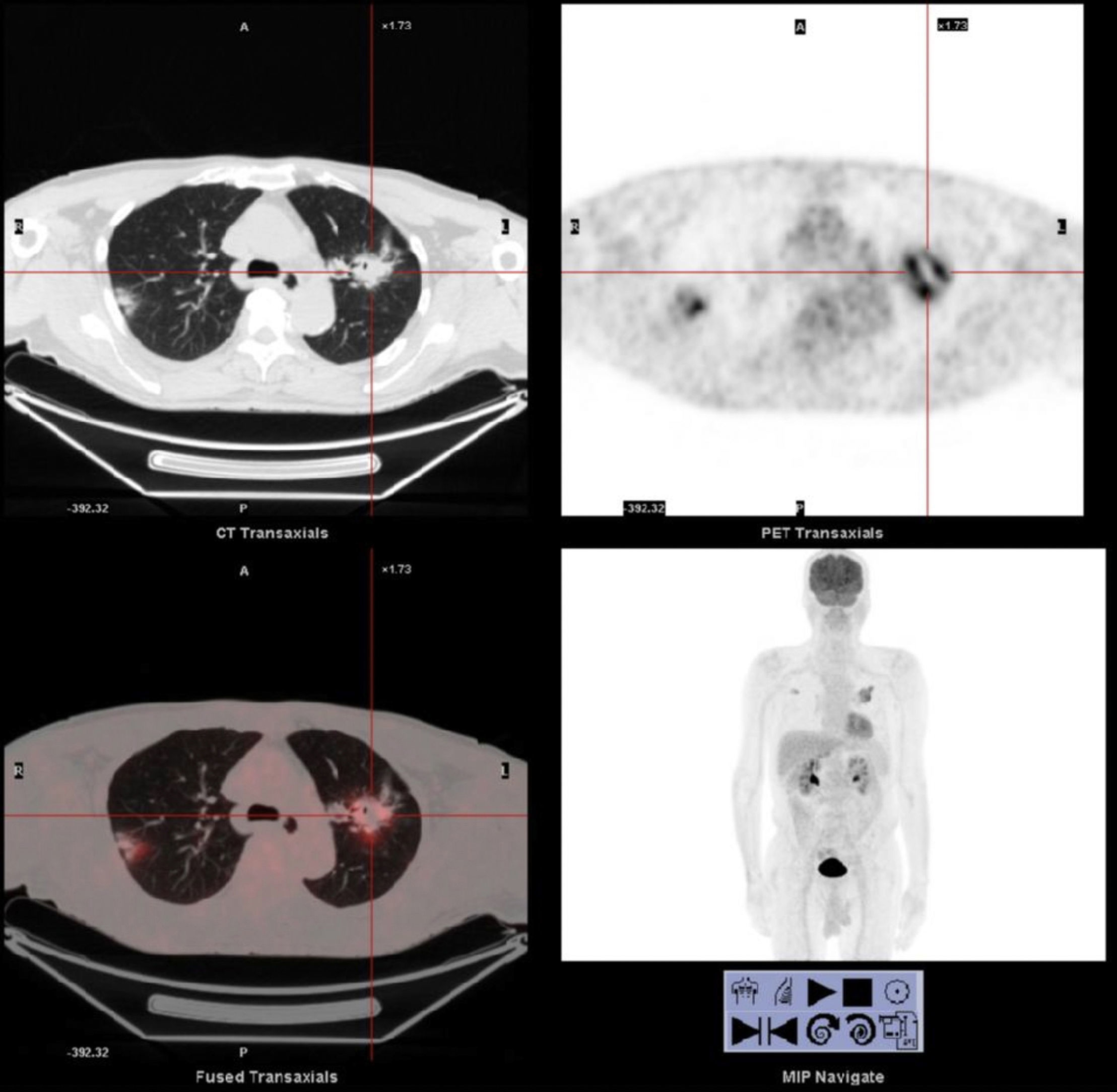
The first case was a 67-year-old female who was admitted with a history of cough and hemoptysis for the last 3 months. The computed tomography of thorax revealed a mass lesion in the left upper lobe of 4.1cm×4.5cm in diameter. The maximum standardized uptake value (SUVmax) of the mass lesion was 13.6 on the PET/CT examination. Other case was a 68-year-old male patient who was admitted with a history of 2 months of cough. The thorax CT revealed a 4cm×2cm mass lesion with spicular radiation in the left upper lobe with a FDG SUVmax of 9.6 in the PET/CT examination (Figs. 1 and 2).


Flexible fiberoptic bronchoscopy was performed in both cases; however, no visible endobronchial lesion was noted. The results of smear and cytology of the bronchial lavage fluid were negative for acid-fast organisms (AFB) and malignant cells. Transthoracic needle biopsy guided by computed tomography was also negative for malignancy. However, culture of bronchial lavage fluid was positive for tuberculosis in both cases.
These data suggested that besides histological evaluation microbiological culture results for mycobacterium should be pursued since a negative result for AFB in sputum and/or bronchial fluid does not rule out the diagnosis of tuberculosis.
In conclusion, the exact role of PET/CT in tuberculosis is not yet clearly defined. We thought that with the development of more specific radiotracers in the future, PET/CT may play a significant role in the diagnosis of tuberculosis.3
Conflict of interestThe authors declare to have no conflict of interest.
