
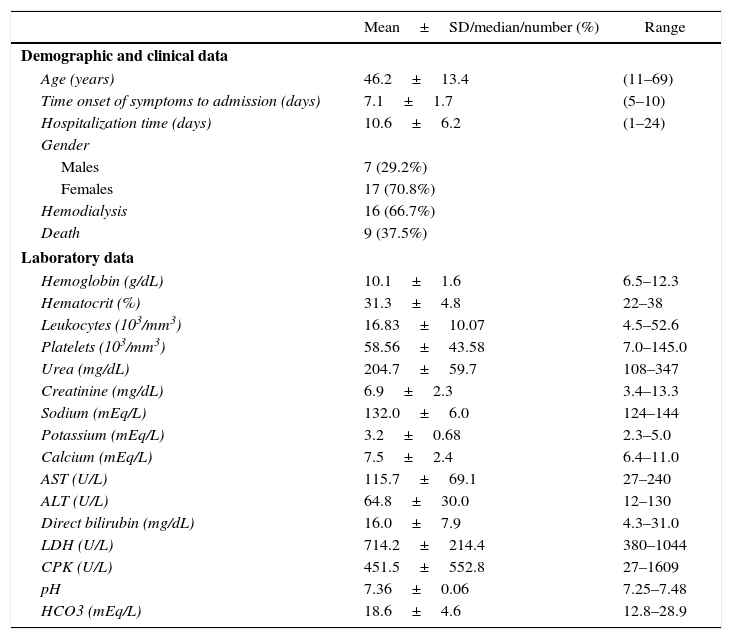
Leptospirosis is a zoonotic disease of global importance and a major public health problem, which is transmitted to humans by contact with mammals’ contaminated urine, most often rats.1 Its severe form manifests as jaundice, acute kidney injury (AKI), and hemorrhage, particularly in the lungs.2 Arrhythmias are the most important cardiac manifestations of this disease, and they have been described as risk factors for death.3 Herein we present clinical, demographic, and laboratory characteristics from a series of patients with leptospirosis admitted to a tertiary hospital in Fortaleza, Ceará, Brazil, from January 1985 to December 2015 who presented AKI and electrocardiographic (ECG) abnormalities. Among 488 leptospirosis patients, 24 (4.91%) presented arrhythmias, 23 acute atrial fibrillations and one atrial flutter. Most of them were young females (17–70.8%). All patients presented severe AKI, 16 (66.7%) needed hemodialysis, and nine patients (37.5%) died. They evidenced thrombocytopenia and high levels of AST, ALT and bilirubin, as summarized in Table 1. The patients were dehydrated on admission, due to vomiting, diarrhea, low fluid intake, polyuria, and excessive transpiration. In addition, hypokalemia, hypocalcemia and metabolic acidosis were noticed. These electrolyte abnormalities may have been a key point in the onset of arrhythmias, since they have been related to ECG abnormalities in leptospirosis, even when there is no myocardial dysfunction.4 Even though serum magnesium values were not available in patients’ charts, we believe that hypomagnesaemia may have also contributed to arrhythmias, as previously reported.5 In summary, dehydration and electrolyte disturbances were crucial to trigger arrhythmias in patients with leptospirosis. Therefore, these factors must be avoided or treated in order to prevent such life-threatening complications.
Demographic, clinical and laboratory data of leptospirosis patients with arrhythmias (n=24).
| Mean±SD/median/number (%) | Range | |
|---|---|---|
| Demographic and clinical data | ||
| Age (years) | 46.2±13.4 | (11–69) |
| Time onset of symptoms to admission (days) | 7.1±1.7 | (5–10) |
| Hospitalization time (days) | 10.6±6.2 | (1–24) |
| Gender | ||
| Males | 7 (29.2%) | |
| Females | 17 (70.8%) | |
| Hemodialysis | 16 (66.7%) | |
| Death | 9 (37.5%) | |
| Laboratory data | ||
| Hemoglobin (g/dL) | 10.1±1.6 | 6.5–12.3 |
| Hematocrit (%) | 31.3±4.8 | 22–38 |
| Leukocytes (103/mm3) | 16.83±10.07 | 4.5–52.6 |
| Platelets (103/mm3) | 58.56±43.58 | 7.0–145.0 |
| Urea (mg/dL) | 204.7±59.7 | 108–347 |
| Creatinine (mg/dL) | 6.9±2.3 | 3.4–13.3 |
| Sodium (mEq/L) | 132.0±6.0 | 124–144 |
| Potassium (mEq/L) | 3.2±0.68 | 2.3–5.0 |
| Calcium (mEq/L) | 7.5±2.4 | 6.4–11.0 |
| AST (U/L) | 115.7±69.1 | 27–240 |
| ALT (U/L) | 64.8±30.0 | 12–130 |
| Direct bilirubin (mg/dL) | 16.0±7.9 | 4.3–31.0 |
| LDH (U/L) | 714.2±214.4 | 380–1044 |
| CPK (U/L) | 451.5±552.8 | 27–1609 |
| pH | 7.36±0.06 | 7.25–7.48 |
| HCO3 (mEq/L) | 18.6±4.6 | 12.8–28.9 |
AST, aspartate aminotransferase; ALT, alanine aminotransferase; LDH, lactate dehydrogenase; CPK, creatine phosphokinase; HCO3, serum bicarbonate.
Variables were expressed as mean±standard deviation.
The authors declare no conflicts of interest.
