
In the antibiotic era, aortic aneurysm is a rare complication of syphilis, what makes the diagnostic assumption even more difficult. Nonetheless, this condition should be suspected in patients with aortic aneurysm. Reports of aortic dissection complicating syphilitic aortitis have been distinctly rare in the literature, and their cause-effect relationship has not been definitely established. In this case report, we present a 62-year-old woman with aortic aneurysm and dissection associated with an unexpected diagnosis of syphilitic aortitis.
Nowadays, aortic aneurysm is a rare complication of syphilis, what makes the diagnostic assumption even more difficult. Nonetheless, this condition can develop and should be suspected in patients with aortic aneurysm. In the antibiotic era, the incidence of late manifestations of syphilis has dramatically declined. Before the discovery of penicillin, tertiary syphilis was the most common cause of thoracic aortic aneurysm, resulting in 5–10% of cardiovascular deaths.1
Reports of aortic dissection complicating syphilitic aortitis have been distinctly rare in the literature,2–7 and their cause–effect relationship has not been definitely established. While it has been proposed that the transverse scars caused by Treponema pallidum infection tight up the layers of the aorta and protect the aorta from dissection, the deposition of mucopolysaccharide in the place of collagen, typical of active syphilitic aortitis, might actually lead to the opposite.3 In this case report, we present a 62-year-old woman with aortic aneurysm and dissection associated with an unexpected diagnosis of syphilitic aortitis.
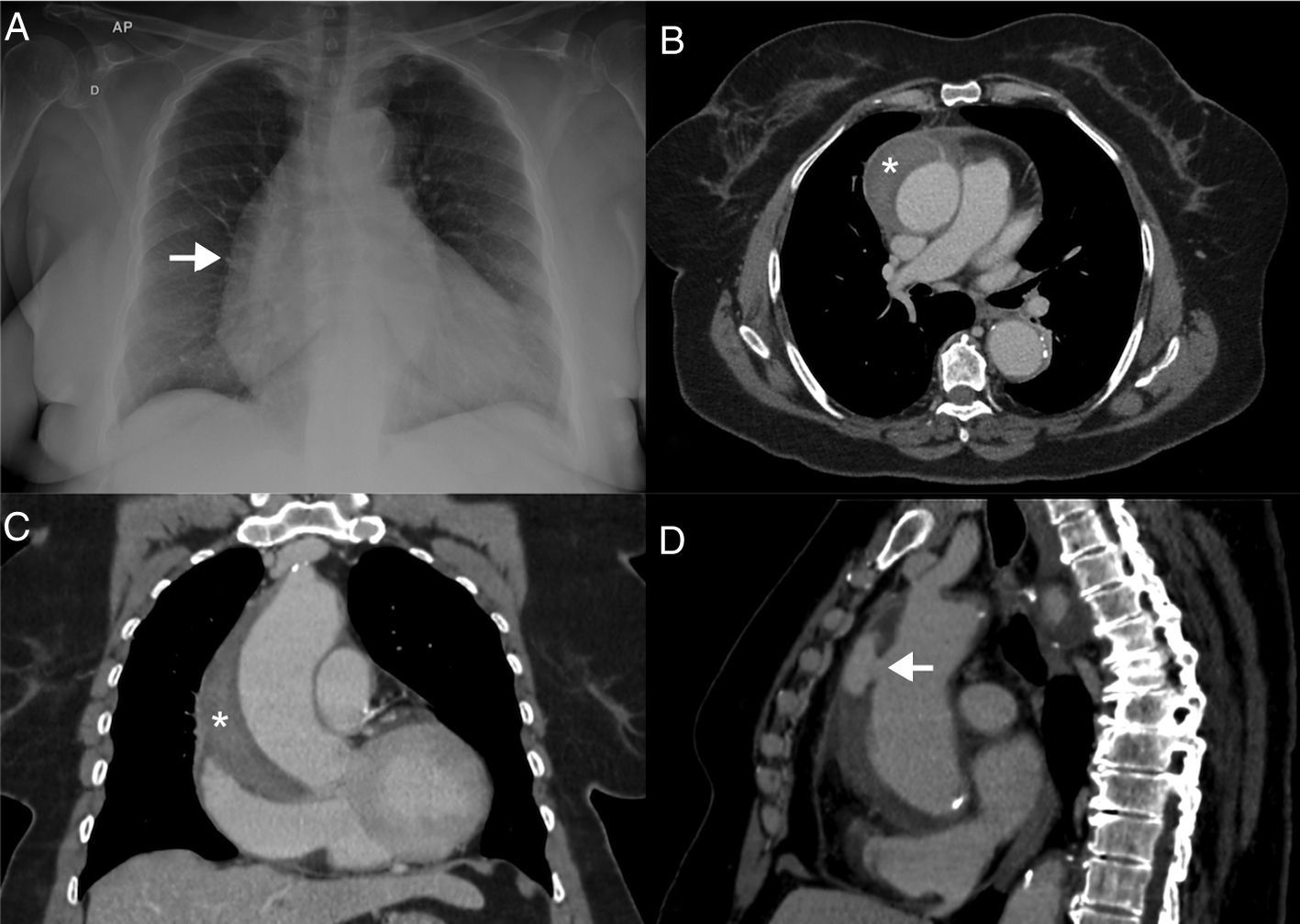
Case reportA 62-year-old woman presented to the emergency department with a history of chest pain with dorsal irradiation that began one week before, followed by subsequent episodes of lesser intensity. Past medical history included hypertension, diabetes mellitus, active smoking (50 packs/year) and grade 2 obesity. Physical examination showed no significant abnormalities on admission. Electrocardiogram evidenced signs of atrial and ventricular overload, secondary repolarization changes and no signs of ischemia. Laboratory evaluation revealed leukocytosis without bandemia (14,700 cells/mm3), troponin within normal limits, C-reactive protein (CRP) 275mg/L (reference: ≤5mg/L) and erythrocyte sedimentation rate (ESR) 113mm (reference: 0–20mm), with no other changes. The chest X-ray showed an increased cardiac area (Fig. 1A).
 shows enlargement of the right heart border. Transaxial, contrast-enhanced computed tomography (B) image showing dilatation of the ascending aorta end evidence of type A aortic dissection (*). Coronal (C) and sagittal oblique (D) contrast enhanced computed tomography images showing a type A aortic dissection (*) and the point of intimal tear (arrow).")
Frontal chest X-ray (A) shows enlargement of the right heart border. Transaxial, contrast-enhanced computed tomography (B) image showing dilatation of the ascending aorta end evidence of type A aortic dissection (*). Coronal (C) and sagittal oblique (D) contrast enhanced computed tomography images showing a type A aortic dissection (*) and the point of intimal tear (arrow).
A contrast-enhanced chest computed tomography (CT) was performed (Fig. 1B–D) and identified a Stanford type A aortic dissection extending to the level proximal to the brachiocephalic trunk. The aorta was dilated (maximum transverse diameter of 6.6cm) and two regions of intimal rupture, both in the distal ascending aorta, were identified. The patient was kept on continuous monitoring in the Intensive Care Unity, aiming to achieve a strict control of blood pressure and heart rate. Syphilis serology was requested, despite the low probability of syphilitic aortitis, revealing negative VDRL and positive fluorescent treponemal antibody-absorption (FTA-ABS) test. The patient denied a previous diagnosis of syphilis or prior treatment for this condition.
Echocardiogram showed mildly increased left atrial volume (41mL/m2; reference: ≤34mL/m2), normal left ventricular diameters, concentric hypertrophy (septum/posterior wall diastolic thickness 13/11mm) and a borderline global systolic function (ejection fraction 53%), without segmental variation. In addition, it also displayed mild aortic regurgitation, ascending aorta dilatation above the sinotubular junction (41mm), and mild to moderate anterior pericardial effusion (10mm thick) without signs suggestive of increased intrapericardial pressure.
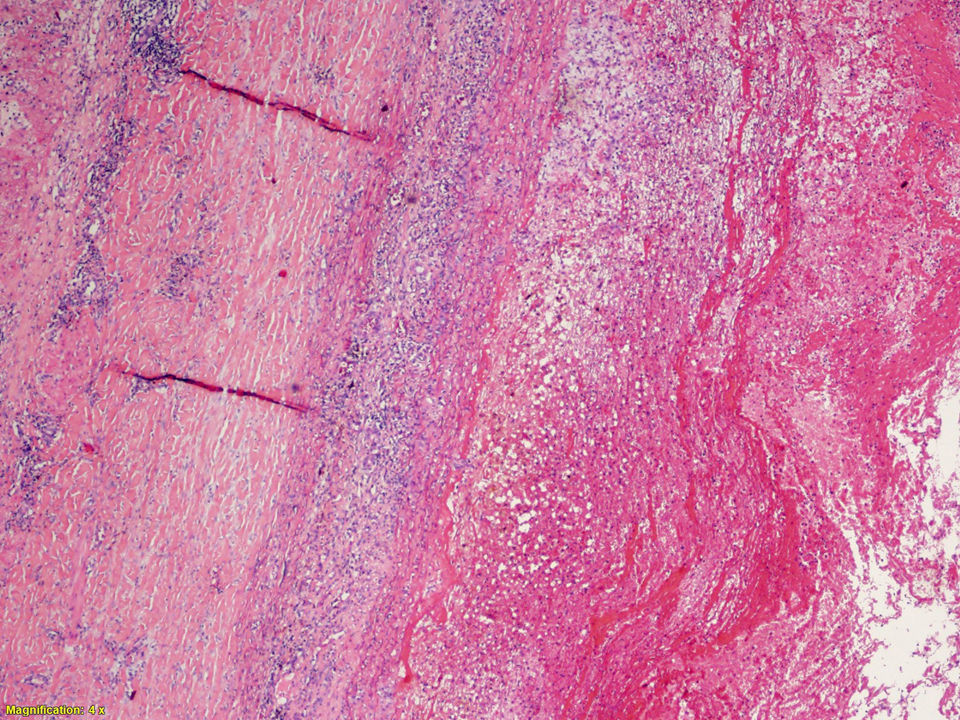
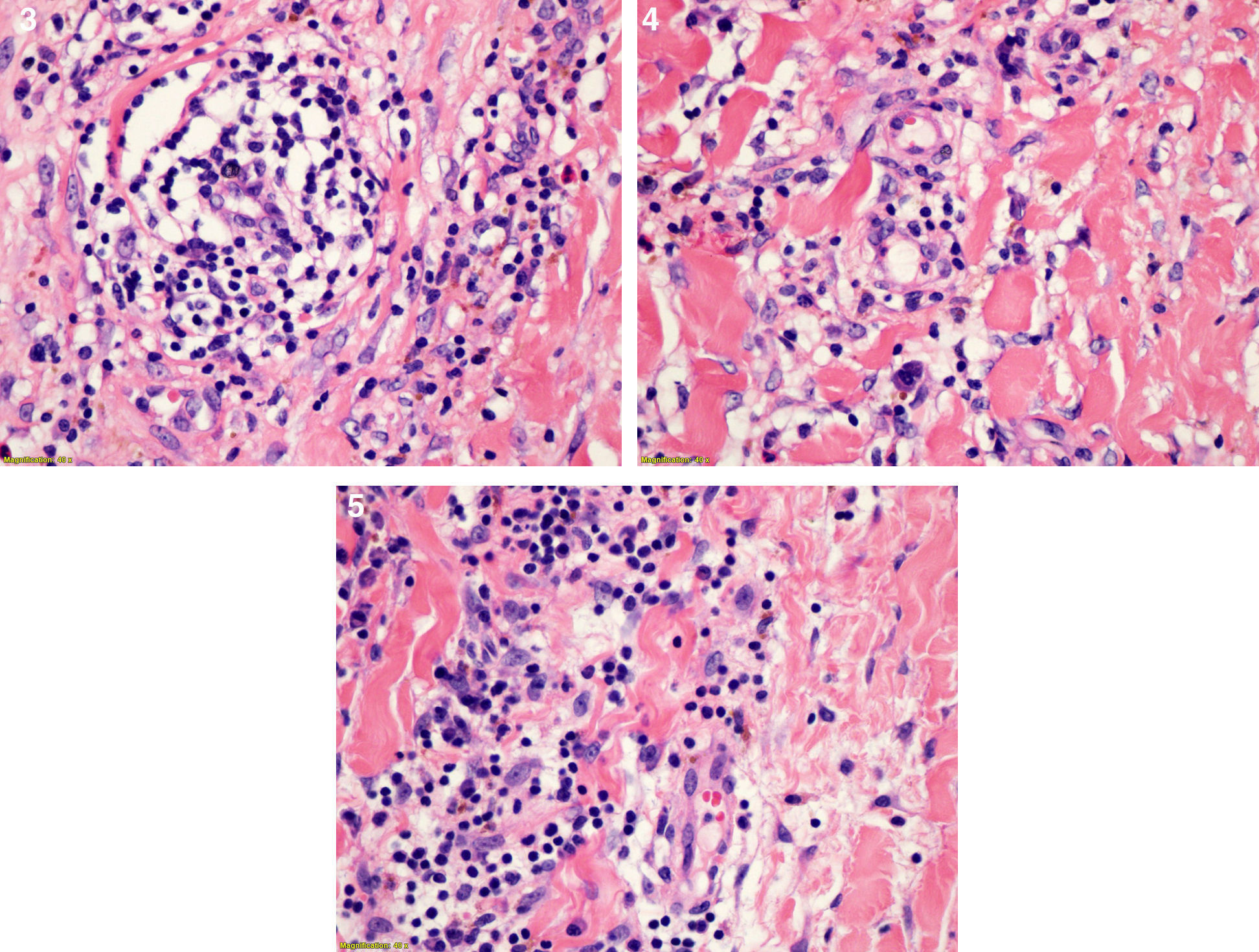
Aortic aneurysmectomy and tube graft interposition was performed. Cinecoronariography carried out before surgery revealed no significant coronary stenosis. Surprisingly, anatomopathological examination of the resected aorta showed acute and chronic inflammation of the artery wall, with necrotic foci and degeneration of the middle layer, typical of syphilitic arteritis (Figs. 2–5). The patient had a good postoperative evolution. Treatment for tertiary syphilis was prescribed with benzathine penicillin G 2.4 million units once weekly for three weeks. Lumbar puncture before treatment showed no central nervous system involvement.
.")
.")
In this case report, an unexpected diagnosis of syphilitic aortitis was performed based on anatomopathological findings and serology. Aortitis is one of the many possible lesions caused by tertiary syphilis. Between all the cardiovascular lesions, aorta injury is the most common. Despite the rarity of the disease, it still exists.8 Nevertheless, tertiary syphilis usually presents within several years to decades after the initiation of latency, but is rare today due to curative antibiotic treatment given for early syphilis or coincidentally for unrelated infections.9
In recent years, significant research has tried to improve the clinical management of syphilis. Despite the promising clinical outcomes data that have been early noticed with the use of azithromycin, molecular resistance to macrolide antibiotics appears to be widespread, and resistance testing of clinical isolates is not readily available in most practice sites. For this reason, routine use of azithromycin cannot be recommended.10 Penicillin, which was first used for treatment of syphilis in the 1940s, has remained the recommended first-line drug for treatment of all stages of syphilis. Unlike most other bacteria, T. pallidum has remained highly sensitive to penicillin. Emergence of penicillin resistance appears unlike since it would presumably require multi-step mutational changes in a bacterium that lacks horizontal gene transfer mechanisms.9
Syphilitic cardiovascular disease occurs more frequently than is recognized clinically.11 Heggtveit2 described that an accurate clinical diagnosis was established in only 17% of a large group of syphilitic aortitis reviewed in a clinicopathological necropsy study. The rarity of this entity makes the diagnosis difficult, mainly because the widespread use of antibiotics, intentional or not prescribed for conditions other than syphilis treatment, decreased the incidence of the disease; in addition, syphilis testing is not routinely requested. In late syphilis, non-treponemal tests like VDRL test and rapid plasma reagin test are less sensitive (71–73%), when compared with treponema-specific tests such as TPHA, microhaemagglutination test and FTA-ABS test (94–96%).1
The basic lesion of cardiovascular syphilis is aortitis. After primary infection, T. pallidum is present in the aortic wall, initially in the adventitia and soon after in the lymphatic vessels. This is one of the main reasons for the tropism of spirochetes to the ascending aorta, since it is rich in lymphatics. The vasa vasorum undergoes a process of endarteritis obliterans, necrosis of medial layer (mesoarteritis), and infiltration of plasma cells. Eventually, the elastic tissue of the vessel is destroyed and replaced by scar tissue. The inflammatory process may continue for a long time and can be found even 25 years after initial infection. The clinical presentation may be of angina (when there is obstruction of the coronary ostia), and/or dyspnea (when there is aortic failure). However, the most common clinical symptom is chest pain secondary to rapid expansion of the syphilitic aneurysm.8
The definitive treatment of aortic aneurysm is surgical repair, which involves resection of the dilated portion of the aorta and replacing it with a synthetic vascular graft. The simultaneous presence of aortic regurgitation or significant coronary disease should be surgically treated at the same time.1 The postoperative treatment with benzathine penicillin, in doses recommended for tertiary syphilis, is regularly implemented to decrease the chances of relapse. However, it is known that even with the elimination of T. pallidum, the chance of recurrence of the disease still persists. Because of this, there is a need for a long-term follow-up of the patient.8
Despite the extremely low prevalence in patients with aortic aneurysm, syphilitic aortitis should always be borne in mind in clinical practice, since this diagnosis have practical implications for the treatment.
Conflicts of interestThe authors declare no conflicts of interest.
