
The impact of central venous catheter (CVC) removal on the outcome of patients with candidemia is controversial, with studies reporting discrepant results depending on the time of CVC removal (early or any time during the course of candidemia).
ObjectiveEvaluate the effect of time to CVC removal, early (within 48h from the diagnosis of candidemia) vs. removal at any time during the course of candidemia, on the 30-day mortality.
MethodsRetrospective cohort study of 285 patients with candidemia analyzing CVC removal within 48h (first analysis) or at any time (second analysis).
ResultsA CVC was in place in 212 patients and was removed in 148 (69.8%), either early (88 patients, 41.5%) or late (60 patients, 28.3%). Overall, the median time to CVC removal was one day (range 1–28) but was six days (range 3–28) for those removed later. In the first analysis, APACHE II score (odds ratio [OR] 1.111, 95% confidence interval [95% CI] 1.066–1.158), removal at any time (OR 0.079, 95% CI 0.021–0.298) and Candida parapsilosis infection (OR 0.291, 95% CI 0.133–0.638) were predictors of 30-day mortality. Early removal was not significant. In the second analysis APACHE II score (OR 1.122, 95% CI 1.071–1.175) and C. parapsilosis infection (OR 0.247, 95% CI 0.103–0.590) retained significance.
ConclusionsThe impact of CVC removal is dependent on whether the optimal analysis strategy is deployed and should be taken into consideration in future analyses.
For years, the management of central venous catheters (CVCs) in patients with candidemia had never been controversial until the publication of two review papers from our group1,2 challenging the international consensus that all CVCs should be removed in all patients with candidemia.3 In the first paper, we showed that the evidence in support of skin (i.e. CVC) as source of candidemia was lacking and provided data strongly suggesting that the primary source was the gut.1 In the second paper, we reviewed 203 studies on candidemia and analyzed the 14 that addressed the impact of CVC removal on survival, concluding that the evidence supporting CVC removal was weak,2 because of several methodological flaws of the published studies, small sample size, lack of multivariate analysis including a validated severity of illness score, and inclusion of patients who died very early before candidemia was diagnosed.
A major controversy in the analysis of CVC removal on the outcome of patients with candidemia is the time of CVC removal. In 2010, we published an analysis of outcome predictors of 892 episodes of candidemia in adult patients. These patients had been enrolled in two randomized controlled trials which were contemporaneous and shared comparable study design.4 Importantly, the data that would allow optimal assessment of the need for and timing of CVC removal had been prospectively collected. We defined early removal as removal within 24 and 48h from treatment initiation while “late removal” referred to removal any time after 48h. Despite the prospective nature of these two clinical trials and their large sample sizes, we could not identify any benefit from “early removal” on any of the six pre-determined meaningful outcomes: treatment response, time to clearance of candidemia, rates of persistent and of recurrent candidemia, and survival 28 and 42 days from diagnosis. Another study analyzed predictors of outcome in patients with candidemia from seven clinical trials.5 Different from our study, in this analysis the time to CVC removal after candidemia, i.e. early vs. late removal, was not taken into consideration. Instead, the analysis focused on whether the CVC was removed or left in place after the diagnosis of candidemia. A strong correlation between CVC removal and survival was observed. As a result, the need for and timing of CVC removal, continued to cause confusion. More importantly, from a biological point of view it is hard to accommodate these two results, i.e., early removal does not impact the outcome but removal at any time (including very late in the course of candidemia) does. These puzzling discrepancies brought us to the following question: do patients survive because their CVC is removed or the CVC is removed because they survive long enough (i.e. favorable host factors)?
In the current manuscript, we analyzed the effect of time to CVC early (within 48h from the diagnosis of candidemia) removal vs. removal at any time, on the 30-day mortality in 285 patients with candidemia. Unique to our study is the application of these two strategies of analysis in the same dataset.
Patients and methodsWe conducted a retrospective analysis of all episodes of candidemia diagnosed at a tertiary care hospital between 1996 and 2013. The setting was a 450-bed university-affiliated hospital located in Rio de Janeiro, Brazil. The study was approved by the Institutional Review Board of the hospital. All data were collected prospectively using a standardized case report form, with a dictionary of terms containing all definitions of underlying conditions and the procedures and treatments performed during the study period. Patients were followed up for 30 days after the incident candidemia or death, whichever came first. An episode of candidemia was defined as an incident isolation of Candida spp. from a blood culture in a patient with clinical signs of infection (fever, hypothermia, hypotension, sepsis). Candidemia occurring >30 days after the date of collection of the first positive blood culture (incident candidemia) was considered a new episode of candidemia. If a patient developed more than one episode of candidemia, only the first episode was considered for this analysis.
Early CVC removal was defined when removal occurred within 48h from the incident candidemia, late removal when CVC was removed >48h of the incident candidemia, and removal at any time (early plus late) during the 30-day period of observation. The primary outcome was 30-day mortality after the incident candidemia. In addition to CVC removal and its timing, the following variables were analyzed as potential factors associated with 30-day mortality: age, sex, APACHE II score (calculated on the day of the incident candidemia), concomitant medical conditions (cancer, diabetes, renal failure, cardiac disease, lung disease, cirrhosis), recent surgery (of any type requiring any anesthesia other than local anesthesia within three months prior to the incident candidemia), dialysis, mucositis, neutropenia (<500neutrophils/mm3), receipt of corticosteroids or total parenteral nutrition within 14 days before the incident candidemia, Candida species, and antifungal drug class (azole, amphotericin B or echinocandin).
Categorical variables were compared between patients who were alive vs. those who were dead by day 30 of the incident candidemia using Chi-square or Fisher's exact tests, as appropriate, and for continuous variables the Wilcoxon test was used. Variables significant at p<0.05 by univariate analysis were included in a stepwise logistic regression analysis (backward and forward). In order to test the effect of the time of CVC removal on the outcome, two models were tested, one including CVC removal at any time as covariate, and the other evaluating early CVC removal. A p-value <0.05 was considered statistically significant. Statistical analyses were performed using SPSS version 15.0 (IBM, Armonk, NY, USA).
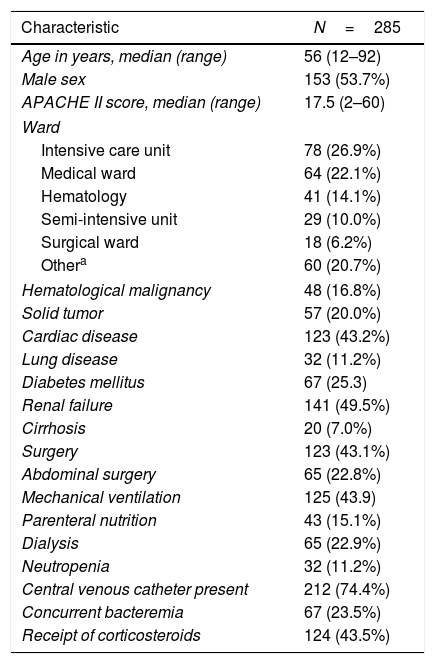
ResultsDuring the study period, 290 episodes of candidemia were diagnosed in 285 patients, with an incidence of 1.27 episodes per 1000 admissions. Five recurrent episodes of candidemia that developed in five patients were excluded. Table 1 shows the characteristics of the 285 episodes of candidemia. The median age was 56 years (range 12–92) and 153 (53.7%) were males. Candida species consisted predominantly of C. albicans (106 cases, 37.2%), C. tropicalis (76, 26.7%), C. parapsilosis (55, 19.3%), and C. glabrata (20, 7.0%). The remaining 28 episodes were caused by C. krusei, C. pelliculosa and C. famata (6 episodes each), C. guilliermondii (4), C. kefyr (3), and C. lipolytica, C. zeylanoides and Pichia ohmeri (1 each).
Baseline characteristics of 285 episodes of candidemia.
| Characteristic | N=285 |
|---|---|
| Age in years, median (range) | 56 (12–92) |
| Male sex | 153 (53.7%) |
| APACHE II score, median (range) | 17.5 (2–60) |
| Ward | |
| Intensive care unit | 78 (26.9%) |
| Medical ward | 64 (22.1%) |
| Hematology | 41 (14.1%) |
| Semi-intensive unit | 29 (10.0%) |
| Surgical ward | 18 (6.2%) |
| Othera | 60 (20.7%) |
| Hematological malignancy | 48 (16.8%) |
| Solid tumor | 57 (20.0%) |
| Cardiac disease | 123 (43.2%) |
| Lung disease | 32 (11.2%) |
| Diabetes mellitus | 67 (25.3) |
| Renal failure | 141 (49.5%) |
| Cirrhosis | 20 (7.0%) |
| Surgery | 123 (43.1%) |
| Abdominal surgery | 65 (22.8%) |
| Mechanical ventilation | 125 (43.9) |
| Parenteral nutrition | 43 (15.1%) |
| Dialysis | 65 (22.9%) |
| Neutropenia | 32 (11.2%) |
| Central venous catheter present | 212 (74.4%) |
| Concurrent bacteremia | 67 (23.5%) |
| Receipt of corticosteroids | 124 (43.5%) |
APACHE, Acute Physiologic and Chronic Health Evaluation.
Antifungal agents were administered in 212 (74.4%) patients. Among the 73 patients who did not receive antifungal therapy, 63 died before the diagnosis of candidemia was made (86.3%). Among the 212 patients treated, fluconazole was the agent most frequently used (122 patients, 57.5%), followed by deoxycholate amphotericin B (56, 26.4%), echinocandins (11, 5.2%), and voriconazole (1 episode only). Twenty-two episodes were treated as part of a randomized double-blind trial (drug unknown).
There were 212 patients (73.1%) with a CVC in place on the day of incident candidemia (182 non-tunneled and 30 tunneled CVCs). The most frequent site of insertion was the jugular vein (87 patients), followed by the subclavian vein (77 patients). Among the 212 patients with CVC, 148 had their CVC removed (69.8%), either early (88 patients, 41.5%) or late (60 patients, 28.3%). Overall, the median time to CVC removal was one day (range 1–28) vs. six days (range 3–28) for those with late removal, including 25 patients whose CVC was not removed until past day 7 of the incident candidemia.
The 30-day mortality rate of the entire cohort was 57.9% and was highest among patients whose CVC was kept in place (93.8%) as compared to the early and late removal groups (55.7% and 40.0%, respectively).
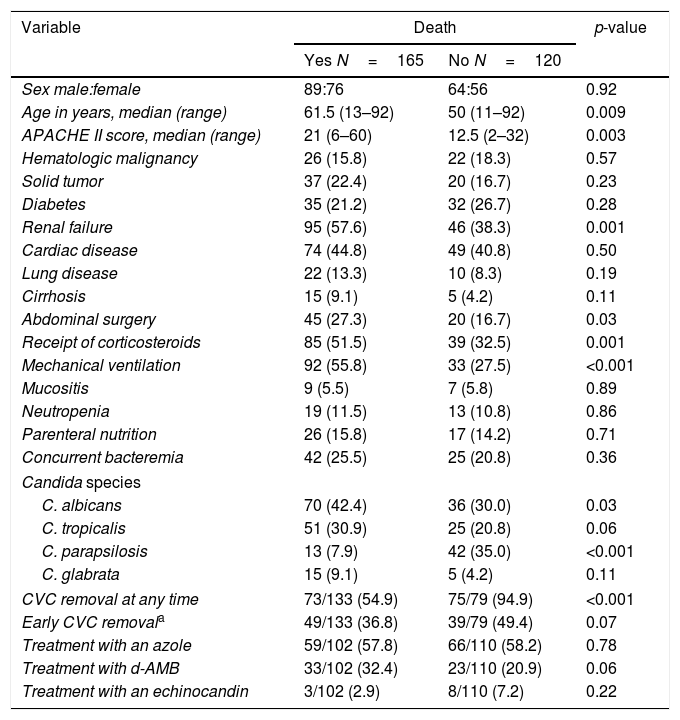
As shown in Table 2, factors associated with 30-day mortality by univariate analysis were older age, higher APACHE II score, renal failure, abdominal surgery, mechanical ventilation, receipt of corticosteroids, and candidemia due to C. albicans. On the other hand, candidemia due to C. parapsilosis and CVC removal at any time were protective, but early removal was not (p=0.07).
Factors associated with 30-day mortality in 285 patients with candidemia by univariate analysis.
| Variable | Death | p-value | |
|---|---|---|---|
| Yes N=165 | No N=120 | ||
| Sex male:female | 89:76 | 64:56 | 0.92 |
| Age in years, median (range) | 61.5 (13–92) | 50 (11–92) | 0.009 |
| APACHE II score, median (range) | 21 (6–60) | 12.5 (2–32) | 0.003 |
| Hematologic malignancy | 26 (15.8) | 22 (18.3) | 0.57 |
| Solid tumor | 37 (22.4) | 20 (16.7) | 0.23 |
| Diabetes | 35 (21.2) | 32 (26.7) | 0.28 |
| Renal failure | 95 (57.6) | 46 (38.3) | 0.001 |
| Cardiac disease | 74 (44.8) | 49 (40.8) | 0.50 |
| Lung disease | 22 (13.3) | 10 (8.3) | 0.19 |
| Cirrhosis | 15 (9.1) | 5 (4.2) | 0.11 |
| Abdominal surgery | 45 (27.3) | 20 (16.7) | 0.03 |
| Receipt of corticosteroids | 85 (51.5) | 39 (32.5) | 0.001 |
| Mechanical ventilation | 92 (55.8) | 33 (27.5) | <0.001 |
| Mucositis | 9 (5.5) | 7 (5.8) | 0.89 |
| Neutropenia | 19 (11.5) | 13 (10.8) | 0.86 |
| Parenteral nutrition | 26 (15.8) | 17 (14.2) | 0.71 |
| Concurrent bacteremia | 42 (25.5) | 25 (20.8) | 0.36 |
| Candida species | |||
| C. albicans | 70 (42.4) | 36 (30.0) | 0.03 |
| C. tropicalis | 51 (30.9) | 25 (20.8) | 0.06 |
| C. parapsilosis | 13 (7.9) | 42 (35.0) | <0.001 |
| C. glabrata | 15 (9.1) | 5 (4.2) | 0.11 |
| CVC removal at any time | 73/133 (54.9) | 75/79 (94.9) | <0.001 |
| Early CVC removala | 49/133 (36.8) | 39/79 (49.4) | 0.07 |
| Treatment with an azole | 59/102 (57.8) | 66/110 (58.2) | 0.78 |
| Treatment with d-AMB | 33/102 (32.4) | 23/110 (20.9) | 0.06 |
| Treatment with an echinocandin | 3/102 (2.9) | 8/110 (7.2) | 0.22 |
Note: N are numbers (%) of patients, unless otherwise indicated. APACHE, Acute Physiologic and Chronic Health Evaluation; CVC, central venous catheter; a within 48h of treatment initiation; d-AMB, deoxycholate amphotericin B.
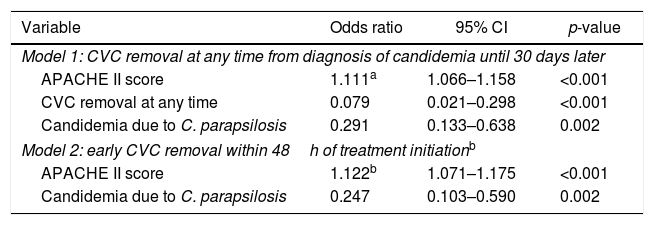
Table 3 shows the two models of multivariate analysis; one included CVC removal at any time as covariate, and the other evaluated early CVC removal. Three variables remained independently associated with mortality in the first model: higher APACHE II score (odds ratio [OR] 1.111, 95% confidence interval [95% CI] 1.066–1.158) was a risk factor for death while CVC removal at any time (OR 0.079, 95% CI 0.021–0.298) and candidemia due to C. parapsilosis (OR 0.291, 95% CI 0.133–0.638) were protective. In the second model, only higher APACHE II score (OR 1.122, 95% CI 1.071–1.175) and candidemia due to C. parapsilosis (OR 0.247, 95% CI 0.103–0.590) remained significant whereas early CVC removal was not.
Factors associated with 30-day mortality in 212 patients with candidemia and a catheter in place (multivariate analysis).
| Variable | Odds ratio | 95% CI | p-value |
|---|---|---|---|
| Model 1: CVC removal at any time from diagnosis of candidemia until 30 days later | |||
| APACHE II score | 1.111a | 1.066–1.158 | <0.001 |
| CVC removal at any time | 0.079 | 0.021–0.298 | <0.001 |
| Candidemia due to C. parapsilosis | 0.291 | 0.133–0.638 | 0.002 |
| Model 2: early CVC removal within 48h of treatment initiationb | |||
| APACHE II score | 1.122b | 1.071–1.175 | <0.001 |
| Candidemia due to C. parapsilosis | 0.247 | 0.103–0.590 | 0.002 |
95% CI, 95% confidence interval; APACHE, Acute Physiologic and Chronic Health Evaluation.
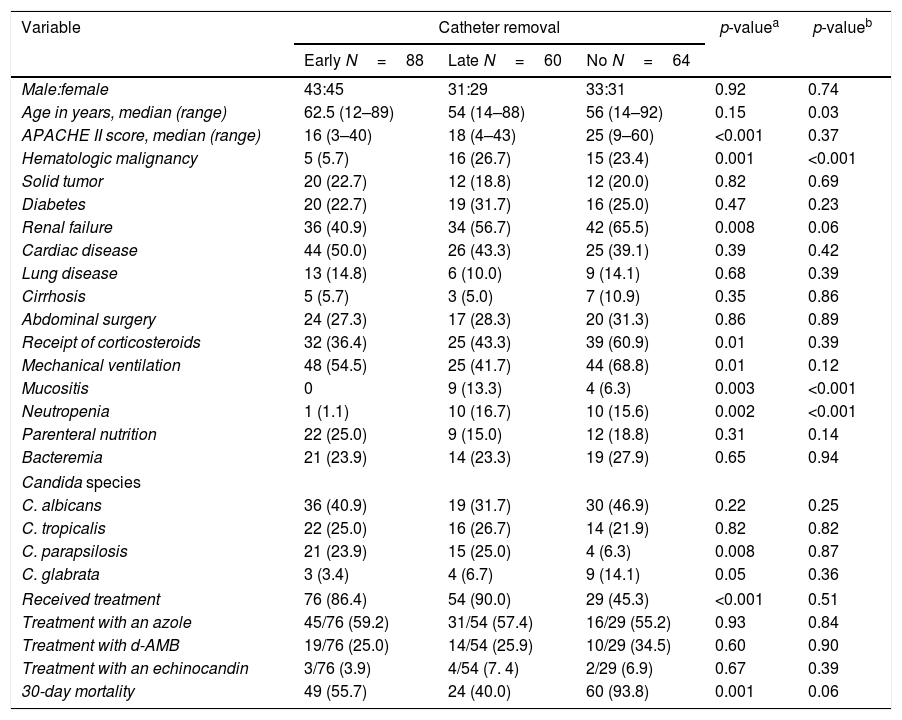
Table 4 shows the characteristics of the 212 patients with a CVC at diagnosis of candidemia according to catheter management (early, late and no CVC removal). Factors associated with no removal included higher APACHE II score, mechanical ventilation, renal failure, receipt of corticosteroids, no antifungal therapy, and non-C. parapsilosis candida species. When early vs. late removal were compared, late removal was associated with younger age, hematologic malignancy, mucositis and neutropenia although only hematologic malignancy remained significant after multivariate analysis (OR 3.349, 95% CI 1.073–10.451, p=0.04).
Characteristics of 212 patients with candidemia according to central catheter management: early, late or no removal during the 30 days of the episode of candidemia.
| Variable | Catheter removal | p-valuea | p-valueb | ||
|---|---|---|---|---|---|
| Early N=88 | Late N=60 | No N=64 | |||
| Male:female | 43:45 | 31:29 | 33:31 | 0.92 | 0.74 |
| Age in years, median (range) | 62.5 (12–89) | 54 (14–88) | 56 (14–92) | 0.15 | 0.03 |
| APACHE II score, median (range) | 16 (3–40) | 18 (4–43) | 25 (9–60) | <0.001 | 0.37 |
| Hematologic malignancy | 5 (5.7) | 16 (26.7) | 15 (23.4) | 0.001 | <0.001 |
| Solid tumor | 20 (22.7) | 12 (18.8) | 12 (20.0) | 0.82 | 0.69 |
| Diabetes | 20 (22.7) | 19 (31.7) | 16 (25.0) | 0.47 | 0.23 |
| Renal failure | 36 (40.9) | 34 (56.7) | 42 (65.5) | 0.008 | 0.06 |
| Cardiac disease | 44 (50.0) | 26 (43.3) | 25 (39.1) | 0.39 | 0.42 |
| Lung disease | 13 (14.8) | 6 (10.0) | 9 (14.1) | 0.68 | 0.39 |
| Cirrhosis | 5 (5.7) | 3 (5.0) | 7 (10.9) | 0.35 | 0.86 |
| Abdominal surgery | 24 (27.3) | 17 (28.3) | 20 (31.3) | 0.86 | 0.89 |
| Receipt of corticosteroids | 32 (36.4) | 25 (43.3) | 39 (60.9) | 0.01 | 0.39 |
| Mechanical ventilation | 48 (54.5) | 25 (41.7) | 44 (68.8) | 0.01 | 0.12 |
| Mucositis | 0 | 9 (13.3) | 4 (6.3) | 0.003 | <0.001 |
| Neutropenia | 1 (1.1) | 10 (16.7) | 10 (15.6) | 0.002 | <0.001 |
| Parenteral nutrition | 22 (25.0) | 9 (15.0) | 12 (18.8) | 0.31 | 0.14 |
| Bacteremia | 21 (23.9) | 14 (23.3) | 19 (27.9) | 0.65 | 0.94 |
| Candida species | |||||
| C. albicans | 36 (40.9) | 19 (31.7) | 30 (46.9) | 0.22 | 0.25 |
| C. tropicalis | 22 (25.0) | 16 (26.7) | 14 (21.9) | 0.82 | 0.82 |
| C. parapsilosis | 21 (23.9) | 15 (25.0) | 4 (6.3) | 0.008 | 0.87 |
| C. glabrata | 3 (3.4) | 4 (6.7) | 9 (14.1) | 0.05 | 0.36 |
| Received treatment | 76 (86.4) | 54 (90.0) | 29 (45.3) | <0.001 | 0.51 |
| Treatment with an azole | 45/76 (59.2) | 31/54 (57.4) | 16/29 (55.2) | 0.93 | 0.84 |
| Treatment with d-AMB | 19/76 (25.0) | 14/54 (25.9) | 10/29 (34.5) | 0.60 | 0.90 |
| Treatment with an echinocandin | 3/76 (3.9) | 4/54 (7. 4) | 2/29 (6.9) | 0.67 | 0.39 |
| 30-day mortality | 49 (55.7) | 24 (40.0) | 60 (93.8) | 0.001 | 0.06 |
Note: N are numbers (%) of patients, unless otherwise indicated. Early removal, within 48h of treatment initiation; Late removal, beyond 48h of treatment initiation. APACHE, Acute Physiologic and Chronic Health Evaluation; d-AMB, deoxycholate amphotericin B.
Our current findings suggest that CVC removal even when performed early,4 is not a key determinant of the outcome of patients with candidemia. Our results that infection with C. parapsilosis is associated with better outcome confirm previously reported results.6 Most importantly, this study shows that the impact of CVC removal is dependent on whether the optimal analysis strategy is deployed.
The rationale behind CVC removal in all patients with candidemia is that the catheter is almost always the source of the infection, and source control is an important component of any therapy. However, this rationale is not evidence-based as we have previously demonstrated.1,2,4
Various studies have evaluated the effect of CVC removal on patient outcome6–24 although many suffered from important analysis biases such as the inclusion of patients who did not have candidemia or patients whose diagnosis of candidemia was made post-mortem, the reliance of univariate analysis only, the omission of key host prognostic variables such as a validated severity of illness score and others. One of such biases was addressed in a recently published study.25 In that study, the authors evaluated the effect of CVC removal on mortality, performing different analyses, taking into consideration if the diagnosis of candidemia was made post-mortem (i.e., the patient was dead by the time blood cultures became positive, and clinicians could decide if CVC should be removed or not). Their conclusion was that CVC retention may be a consequence rather than a cause of unfavorable outcome.
Perhaps most importantly is the lack of information on the day of CVC removal after candidemia which allows us to determine whether the currently advocated “removal as early as possible” is supported by the evidence. As an example, the CVC could have been removed on day eight after initiation of treatment, and the survival benefit is likely attributed to the fact that these patients were still alive on that day to have their catheter removed. Indeed, in our cohort, the median time to removal for the late removal group was six days (range 3–28 days), and was beyond seven days for more than 40% of these patients. Notably, a higher mortality rate was observed among the “early removal” as compared to the “late removal group” (56.2% vs. 38.7%, respectively), strongly suggesting that patients had their CVC removed because they survived long enough (i.e. favorable host factors) and not the opposite, i.e. they survived because their CVC was removed.
On a more practical level, the recommendation for early removal of CVCs in all instances is very difficult to implement because most patients with candidemia may be severely ill, thrombocytopenic and have more than one CVC which begs the following questions: which CVCs should be first removed and why; when should the second CVC be taken out and on what basis and how safe is it to insert another CVC in such critically ill patients. The difficulty in following this recommendation is illustrated in a randomized trial of treatment of candidemia comparing micafungin with liposomal amphotericin B,26 in which CVC removal at baseline (before treatment initiation) was required per protocol. Yet, this was performed in only 142 of 277 patients (51%) despite the fact that keeping the CVC was a protocol deviation.
In 2010, we published the first study in which we asked the question of whether “early” CVC removal affected outcomes based on the concept that if catheter removal was an effective therapeutic strategy, it had to be instituted as early as possible.4 Unique to that dataset were the multicenter-multinational enrolment, the large sample size, the prospective and standardized evaluation of treatment response, the per protocol requirement for obtaining daily blood cultures in order to document the time of eradication of candidemia, and the recording of the actual date of CVC removal. These features allowed us to run a robust analysis of 842 episodes of candidemia and evaluate the effect of early CVC removal (two time points, within 24 and 48h of treatment initiation) on six pre-defined endpoints: overall treatment success, 28- and 42-day survival, rates of persistent or recurrent candidemia, and time to mycological eradication. Despite the robustness of this prospective data set, we could not identify a beneficial effect for early removal of the CVC on any of these predefined outcomes.4
Since our publication, two studies analyzed the effect of early CVC removal on the outcome of patients with candidemia. The first was a population-based survey conducted in 29 Spanish hospitals including 752 episodes of candidemia. By multivariate analysis, early CVC removal (within 48h from the incident candidemia) was associated with lower chance of early (0–7 days from incident candidemia) but not late (8–30 days) mortality.27 Unfortunately, no severity of illness score was included in the analysis, i.e. key host variables were not adjusted for, which represents a major limitation. Another report was a prospective analysis of 229 episodes of candidemia in a single-center, and found that early CVC removal had a protective effect on survival.28 Some differences between this study and ours may explain the discrepant results, including the time point for survival (during hospitalization as opposed to 30 days in our study), no analysis of C. parapsilosis candidemia as a covariate, and the use of Cox regression instead of logistic regression in the multivariate analysis.
In the present study, we asked whether the impact of CVC removal on outcome was dependent on the analysis strategy, using exactly the same database. As expected, CVC removal at any time was strongly associated with a better outcome but early CVC removal was not significant, even in univariate analysis. In the “early removal” strategy, the outcome was predicted by the well-known host prognostic factors (APACHE II score)4,6,7,14,29 and by candidemia due to C. parapsilosis.6
How can we accommodate these two conflicting paradigms in the same equation? Reflecting on biological plausibility, if CVC removal was key to managing a patient with candidemia (together with prompt initiation of appropriate antifungal therapy), one should expect that the earlier it was instituted the better the outcome. However, the lack of a survival benefit of early CVC removal argues against the adoption of this strategy. On the other hand, if early CVC removal does not impact outcome, what is the biological plausibility that late CVC removal would? The data presented here suggest that the observed beneficial effect of late CVC removal is not biologically plausible, but just a methodological trap.
Based on the present data, what would be the best strategy at the bedside? We believe that the individual approach that we proposed in our papers published in 2002 and 2010 still stand2,4: if there is no infection at the site of the CVC, start treatment, and consider removing the CVC if the patient does not improve.
Our study has some important limitations, including its retrospective nature and the fact that it is a single-center study with a relatively small sample size. In addition, changes in antifungal armamentarium and therapies over the study period may have impacted the outcome. Nevertheless, the main objective of the study was to bring up a methodologic discussion in the analysis of CVC removal rather than definitively establish the optimal strategy.
In conclusion, the impact of CVC removal on 30-day mortality seems to be influenced by the analysis strategy. Studies analyzing this variable should take into consideration the actual time of CVC removal.
Conflicts of interestThe authors declare no conflicts of interest.
