
HIV-1 mother-to-child transmission (HIV-1 MTCT), is an important cause of children mortality worldwide. Brazil has been traditionally praised by its HIV/Aids program, which provides free-of-charge care for people living with HIV-1. Using public epidemiology and demographic databases, we aimed at modeling HIV-1 MTCT prevalence in Brazil through the years (1994–2016) and elaborate a statistical model for forecasting, contributing to HIV-1 epidemiologic surveillance and healthcare decision-making. We downloaded sets of live births and mothers’ data alongside HIV-1 cases notification in children one year old or less. Through time series modeling, we estimated prevalence along the years in Brazil, and observed a remarkable decrease of HIV-1 MTCT between 1994 (10 cases per 100,000 live births) and 2016 (five cases per 100,000 live births), a reduction of 50%. Using our model, we elaborated a prognosis for each Brazilian state to help HIV-1 surveillance decision making, indicating which states are in theory in risk of experiencing a rise in HIV-1 MTCT prevalence. Ten states had good (37%), nine had mild (33%), and eight had poor prognostics (30%). Stratifying the prognostics by Brazilian region, we observed that the Northeast region had more states with poor prognosis, followed by North and Midwest, Southeast and South with one state of poor prognosis each. Brazil undoubtedly advanced in the fight against HIV-1 MTCT in the past two decades. We hope our model will help indicating where HIV-1 MTCT prevalence may rise in the future and support government decision makers regarding HIV-1 surveillance and prevention.
The human immunodeficiency virus type 1 (HIV-1) is a retrovirus that infects T CD4+ lymphocytes, resulting in a progressive deterioration of the immune system, leading to acquired immunodeficiency syndrome (Aids), if the infection is left undiagnosed and untreated with antiretroviral drugs. HIV-1 transmission occurs through unprotected sexual intercourse, blood transfusions and needle sharing, and through an HIV-1 infected mother to her child during pregnancy or breastfeeding.1 HIV-1 mother-to-child transmission (HIV-1 MTCT), also known as vertical or perinatal transmission, is an important cause of child mortality, and it is estimated that about two million children are infected with HIV-1 worldwide.2 Use of antiretroviral drugs during pregnancy is essential for HIV-1 MTCT prevention. The rate of transmission without treatment ranges between 15% and 45%, falling below 2% with proper treatment with plasma HIV-1 suppression to undetectable levels.3
Brazil has been traditionally praised by its HIV-1/Aids program, which provides free-of-charge and universal prevention tools, diagnostic tests, and care for people living with HIV-1 in the public healthcare network, known as SUS (Sistema Único de Saúde).4 In the last few years, Brazil increased HIV-1 testing coverage among pregnant women.5 Thus, we aimed to model HIV-1 MTCT prevalence in Brazil through the years and elaborate a statistical model for forecasting, contributing to HIV-1 epidemiologic surveillance and healthcare decision-making.
MethodsData collection and manipulationTo estimate HIV-1 MTCT history in Brazil, we downloaded two sets of data from DATASUS, which is a public database that integrates live births, causes of death, compulsory notification comorbidities (such as HIV-1 infection and Aids cases) and demographic data.6 The first dataset contained the number of all HIV/Aids cases detected among Brazilian individuals aged one year or less, according to federative unit (26 states and a Federal District) and year of diagnosis, ranging from 1994 to 2016. This first dataset represented the probable cases of HIV-1 MTCT, as we assumed that children in this age group were probably diagnosed with the infection within their year of birth. In other words, the year of diagnosis = year of birth.
The second dataset contained the number of all live births, also according to Brazilian region, federative unit and year of diagnosis, in addition to information about the mothers: race (white, black, admixed, Asiatic descent and indigenous descent, respectively following the classification of Brazil’s demographic council, IBGE),7 age at the time of delivery (10–14, 15–19, 20–24, 25–29, 30–34, 35–39, 40–44, 45–49, 50–54, and 55 or more years old), type of delivery (vaginal or cesarean section), number of prenatal consultations (zero, one to three, four to six and seven or more consultations), and educational level (zero, one to three, four to seven, eight to 11 and 12 or more years of education).
To simplify the analysis, we dichotomized the variables race, age, educational level and number of prenatal consultations level and summed the respective counts into new categories. Race was modeled with the categories “white” or “non-white”, age at delivery with “less than 25 years old” or “25 years old or more”, education with “no formal education” or “any years of education”, and number of prenatal consultations with “ideal number of consultations (seven or more)” or “suboptimal number of consultations (less than seven)”.
Using the number of infected children from the first dataset as numerator and all live births from the second dataset as denominator after excluding missing data, we estimated the prevalence of HIV-1 MTCT per 100,000 live births per year, hereafter termed “HIV-1 MTCT prevalence” and it was our variable of interest. The explanatory variables were also converted this way, giving a profile of the mothers having children each year according to their federative unit and nationwide Brazil.
Statistical analysisAll statistical analyses were performed with R software version 3.5.1.8 All analyses were two-tailed and level of significance (α) was set at 5%.
Linear regression analysisWith the per 100,000 live births data, we performed linear regression analysis using the base R package stats8 to check if any of the mother’s characteristics were associated with HIV-1 MTCT prevalence. For this analysis, we used nationwide (aggregated for Brazil as a whole) data.
Time series analysisWe described Brazil’s HIV-1 MTCT prevalence through time series analysis using the R packages tseries9 and forecast.10
We then considered ARIMAX (autoregressive integrated moving average – ARIMA – with exogenous inputs) models to forecast values of HIV-1 MTCT prevalence at both national and state levels. Briefly, an ARIMAX model is a type of ARIMA model with external predictors. On the other hand, an ARIMA model is a time series model that represents linear phenomena that appear to be stationary – a series of values ordered in time for which its present values depend only on their past values and random noise (with mean equal to zero and constant variance), hence the term “moving average”. The “autoregressive” term means that the interest variable values are a regression of present against past values. The “integrated” term indicates that the data values can be replaced with the difference between their present and past values. The general representation of an ARIMA model is the denotation ARIMA(p, d, q), in which p represents the number of autoregressive parameters of the model, d represents the number of differencing steps necessary to remove any non-stationarity, and q represents the number of parameters related to the moving averages.11 An ARIMAX model therefore permits the inclusion of explanatory variables (in our case, the mother’s characteristics as mentioned above) that could be useful for improving the forecast of the variable of interest (HIV-1 MTCT prevalence).12
We then selected the best predictive model based on the collected data according to the “auto.arima” algorithm from the forecast package, which considers several models and automatically returns a stationary model with the smallest Akaike Information Criterion (AIC) value, meaning it had the best fit to the data.13
More specifically, we produced 28 time series models. The first was made using nationwide data (the Brazil model) and the remaining 27 were made using data from each Brazilian federative unit. In each prediction we included the best external predictors as indicated by correlation analysis to improve the predictive power of the time series models.
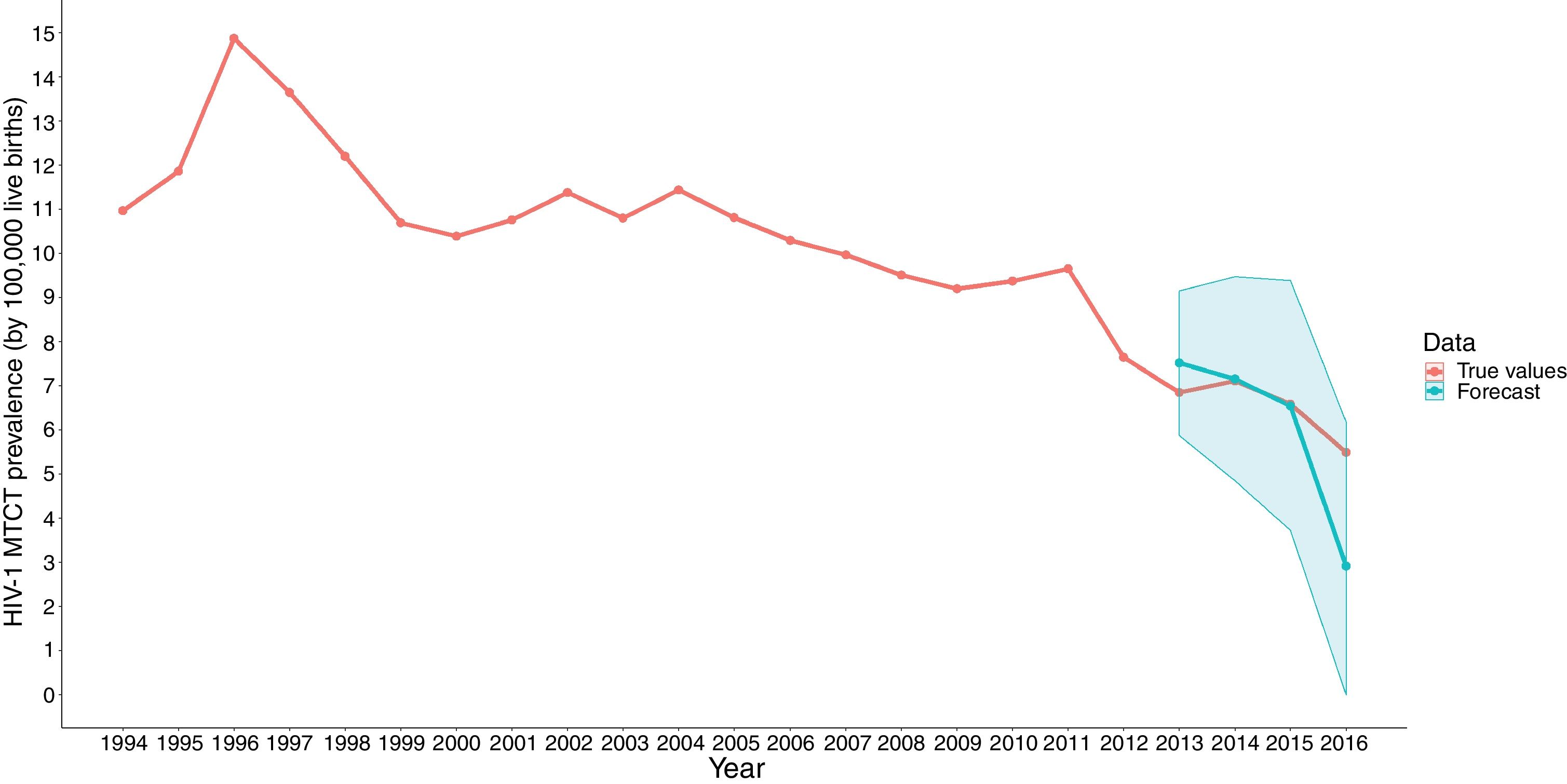
The model outputs were extracted with the package dplyr.14 The plots for each model were made using packages, ggplot215 and ggforce.16 Briefly, time series are a sequence of observations ordered in time.17 With these models, we aimed at predicting HIV-1 MTCT prevalence using data collected between 1994 and 2016. To test the fit of the models, we used only the data between 1994 and 2012 for modeling and then compared the predictions with their respective 95% confidence intervals the actual observations (“true” values) through plots for each time series.
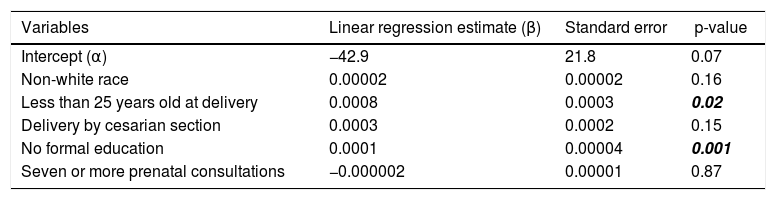
ResultsThe estimated HIV-1 MTCT prevalence in Brazil decreased to five cases per 100,000 live births in 2016 from 10 cases per 100,000 cases in 1994 (Fig. 1), a 50% decrease. The correlation analysis pointed that mothers’ low educational level and being younger than 25 years at delivery were significantly associated with HIV-1 MTCT prevalence increase (p = 0.02 and p = 0.001, respectively). Race (p = 0.16), type of delivery (p = 0.15), and number of prenatal consultations (p = 0.87) did not influence prevalence. The regression model had an adjusted R2 = 0.88 and it was statistically significant (F-statistic = 34.0 on five and 17 degrees-of-freedom, p-value << 0.001). Therefore, these variables were used as external predictors for the ARIMAX models (Table 1).

Multiple linear regression model for explanatory variables selection used in time series modeling.
| Variables | Linear regression estimate (β) | Standard error | p-value |
|---|---|---|---|
| Intercept (α) | −42.9 | 21.8 | 0.07 |
| Non-white race | 0.00002 | 0.00002 | 0.16 |
| Less than 25 years old at delivery | 0.0008 | 0.0003 | 0.02 |
| Delivery by cesarian section | 0.0003 | 0.0002 | 0.15 |
| No formal education | 0.0001 | 0.00004 | 0.001 |
| Seven or more prenatal consultations | −0.000002 | 0.00001 | 0.87 |
The bold italic values are statistically significant values (level of significance alpha=0.05) in a multiple linear regression model.
The ARIMAX models forecast for years 2013, 2014, 2015, and 2016 generally had good fit to the data, as demonstrated by the 95% confidence intervals, which covered the true observations, as displayed in Fig. 1, for example. The only exception was the forecast for Alagoas state, in which the true values were well above the forecast values. Remarkably, Alagoas is the Brazilian state with the lowest human development index, HDI = 0.631. For comparison, Brazil’s HDI is 0.754.7 Thus, government underfunding may be associated with the predicted rise of HIV-1 MTCT prevalence. The 27 plots for each federative unit are available in Supplementary Fig. 1. Additionally, some forecasts yielded negative values, so we replaced them with zero, since prevalence values cannot be negative.
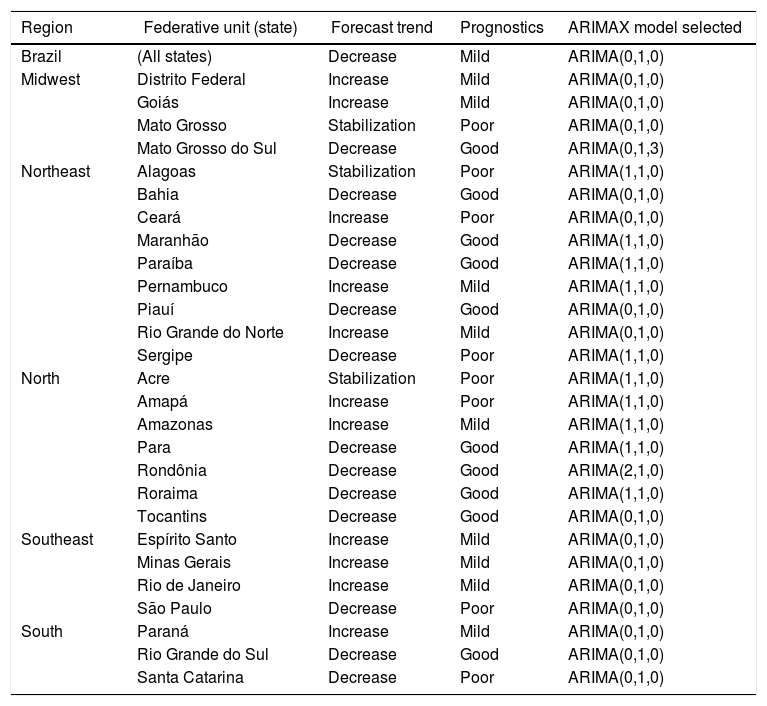
We compared the estimated prevalence values (“true” values) with the values provided by each forecast. These values are reported in Supplementary Table 1 and elaborated a tentative “prognostic” regarding HIV-1 MTCT prevalence behavior in Brazil and each federative unit. We termed a “good” prognostic if (1) the forecast indicated a decreasing trend in the prevalence AND (2) the “true” values were lower than the predicted. A “mild” prognostic was defined as (1) the forecast indicated a stabilizing or increasing trend in the prevalence AND (2) the “true” values were lower than the predicted. Finally, a “poor” prognostic was deemed when (1) the forecast indicated a stabilizing or increasing trend in the prevalence OR decreasing trend AND (2) the “true” values were higher than the predicted. Results of this rationale are summarized on Table 2.
Results summary for ARIMAX models for Brazil’s HIV-1 MTCT prevalence forecasting (years 2013–2016). Regions and federative units (states) are listed alphabetically.
| Region | Federative unit (state) | Forecast trend | Prognostics | ARIMAX model selected |
|---|---|---|---|---|
| Brazil | (All states) | Decrease | Mild | ARIMA(0,1,0) |
| Midwest | Distrito Federal | Increase | Mild | ARIMA(0,1,0) |
| Goiás | Increase | Mild | ARIMA(0,1,0) | |
| Mato Grosso | Stabilization | Poor | ARIMA(0,1,0) | |
| Mato Grosso do Sul | Decrease | Good | ARIMA(0,1,3) | |
| Northeast | Alagoas | Stabilization | Poor | ARIMA(1,1,0) |
| Bahia | Decrease | Good | ARIMA(0,1,0) | |
| Ceará | Increase | Poor | ARIMA(0,1,0) | |
| Maranhão | Decrease | Good | ARIMA(1,1,0) | |
| Paraíba | Decrease | Good | ARIMA(1,1,0) | |
| Pernambuco | Increase | Mild | ARIMA(1,1,0) | |
| Piauí | Decrease | Good | ARIMA(0,1,0) | |
| Rio Grande do Norte | Increase | Mild | ARIMA(0,1,0) | |
| Sergipe | Decrease | Poor | ARIMA(1,1,0) | |
| North | Acre | Stabilization | Poor | ARIMA(1,1,0) |
| Amapá | Increase | Poor | ARIMA(1,1,0) | |
| Amazonas | Increase | Mild | ARIMA(1,1,0) | |
| Para | Decrease | Good | ARIMA(1,1,0) | |
| Rondônia | Decrease | Good | ARIMA(2,1,0) | |
| Roraima | Decrease | Good | ARIMA(1,1,0) | |
| Tocantins | Decrease | Good | ARIMA(0,1,0) | |
| Southeast | Espírito Santo | Increase | Mild | ARIMA(0,1,0) |
| Minas Gerais | Increase | Mild | ARIMA(0,1,0) | |
| Rio de Janeiro | Increase | Mild | ARIMA(0,1,0) | |
| São Paulo | Decrease | Poor | ARIMA(0,1,0) | |
| South | Paraná | Increase | Mild | ARIMA(0,1,0) |
| Rio Grande do Sul | Decrease | Good | ARIMA(0,1,0) | |
| Santa Catarina | Decrease | Poor | ARIMA(0,1,0) |
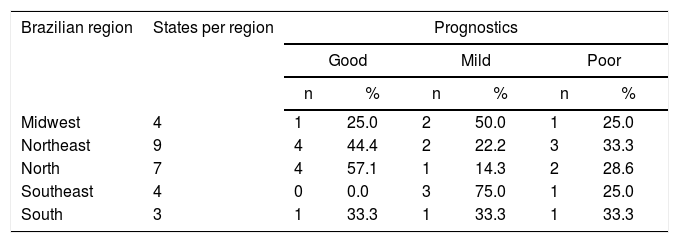
Ten states had good (37%), nine had mild (33%), and eight had poor prognostic (30%). Stratifying the prognostics by Brazilian region, we observed that the Northeast region had the most states with poor prognosis (three states, a third of the states in the region: Alagoas, Ceará, and Sergipe), followed by North region (two states in a region with seven states: Acre and Amapá). The Midwest, (four states), Southeast (four states), and South (three states) had one state with poor prognosis each (Mato Grosso, São Paulo, and Santa Catarina, respectively) (Table 3).
Summary of HIV-1 mother-to-child transmission forecast prognosis, stratified by Brazilian region.
| Brazilian region | States per region | Prognostics | |||||
|---|---|---|---|---|---|---|---|
| Good | Mild | Poor | |||||
| n | % | n | % | n | % | ||
| Midwest | 4 | 1 | 25.0 | 2 | 50.0 | 1 | 25.0 |
| Northeast | 9 | 4 | 44.4 | 2 | 22.2 | 3 | 33.3 |
| North | 7 | 4 | 57.1 | 1 | 14.3 | 2 | 28.6 |
| Southeast | 4 | 0 | 0.0 | 3 | 75.0 | 1 | 25.0 |
| South | 3 | 1 | 33.3 | 1 | 33.3 | 1 | 33.3 |
We performed a time series modeling of HIV-1 MTCT prevalence evolution in Brazil between 1994 and 2016, aiming to forecast this prevalence for future years, based on the demographic characteristics of childbearing women (race, age, type of delivery, educational level, and number of prenatal consultations received).
We observed a significant association between delivery at younger age and low educational level with prevalence of HIV-1 MTCT, agreeing with the available evidence that in Brazil, the majority of HIV-1 infection cases occur among poorer individuals, with less access to education (“pauperization” of the epidemics).18 Thus, it is logical to think that these women that are at higher risk of carrying pregnancies while undiagnosed by the infection. The untreated infection is strongly associated with the risk to HIV-1 MTCT.2
Between 1996 and 2012, Brazil invested US$ 1.6 billion for the provision of universal, free-of-charge, antiretroviral care and general healthcare for people living with HIV-1. This investment payed off: there was a remarkable reduction of mortality and morbidity related with HIV-1 infections and provided an estimated US$ 2 billion economy in hospitalizations.19 Moreover, Brazil also enacted healthcare policies that guarantee free HIV-1 rapid tests and substitutes for maternal milk for pregnant and breastfeeding women. Since 2012, pregnant women are offered antiretroviral treatment regardless of CD4 + T cell count and continue treatment after childbirth.4
Consequently, according to our estimates, Brazil cut by half the rate of new perinatal HIV-1 infection in the past two decades. Currently, with an estimated five infections per 100,000 live births, it is a promising candidate for reaching the World Health Organization goals of elimination of HIV-1 MTCT.20 For comparison, the more realistic goal set by the USA Centers for Disease Control (CDC) is less than 1 infection per 100,000 live births, since eliminating HIV-1 MTCT is very difficult, since women can still be infected, as the pandemics is still ongoing.21 The Brazilian Ministry of Health is actively committed to the attainment of this goal, promoting initiatives such as certification of municipalities and states that achieve incidence rates of 0.3 new cases or less cases in the past three years and a prevalence of 2% of infected children among the exposed to HIV-1 in the past three years.22
Our forecast pointed to a further reduction in the Brazilian HIV-1 MTCT prevalence, but the actual values were higher than the predictions in the final year of the time series, 2016. Therefore, we suppose that there is some yet unidentified factor contributing to slow down deceleration in the prevalence. One of those could be the recent spike of new HIV-1 cases among younger individuals. For example, there was a 13.4% increase in the number of HIV-1 detections among women aged between 15 and 19 years when comparing the years of 2006 and 2016.5 Therefore, if more women in the start of their childbearing age are being infected, it is expected that some of these infections can be transmitted to their future children.
Our study has some limitations. Since we worked with secondary data, we are subject to their inescapable problems, such as missing information and sub-notification. Nevertheless, we believe that we have been able to capture important trends in HIV-1 MTCT in Brazil. Moreover, it is possible that the number of prenatal consultations and delivery by cesarian section were not significantly associated with HIV-1 MTCT during our multiple linear regression model during explanatory variables selection for time series modeling due to suboptimal data in the consulted DATASUS registry. Proper prenatal care is obviously a powerful tool against HIV-1 MTCT, reducing perinatal HIV transmission probability to less than 1%.23 A previous study regarding the New York state (USA) investment in prenatal care of HIV-1 infected pregnant women estimated that “for every $1 invested in preventing perinatal HIV infections, almost $4 in HIV treatment costs have been saved”. It is important to point out that we included this variable in our model despite not achieving strictly statistical association.
ConclusionBrazil undoubtedly advanced in the fight against HIV-1 as well as in HIV-1 MTCT care in the past two decades, providing universal treatment for all people living with HIV-1 and reducing HIV-1 MTCT prevalence. We elaborated a time series statistical model with the intention to continuously improve these efforts, indicating where HIV-1 MTCT prevalence may rise in the future, which is undesirable, and we hope that it could help government decision making regarding HIV-1 surveillance and prevention.
FundingThis work was supported by Fundação de Amparo à Ciência e Tecnologia de Pernambuco, FACEPE (A.V.C.C, scholarship grant number BFP-0018-2.02/17).
Conflicts of interestThe authors declare no conflicts of interest.
The following are Supplementary data to this article:
