
A new point-of-care HIV viral load, mPIMA HIV-1/2 VL, Abbott, USA, has been recently developed. This point-of-care viral load requires no skilled person to run and uses a small plasma volume (50μL). However, obtaining 50μL of plasma can be a challenge in limited resource settings. We validated a simple and easy method to obtain enough amount of plasma to run a point-of-care viral load. The study utilized 149 specimens from patients failing antiretroviral therapy. At least 250μL of whole blood was collected in a microtube/EDTA from fingerstick (fs-plasma) and immediately centrifuged. Parallel collection of venous blood to obtain plasma (vp-plasma) was used to compare performance in a point-of-care viral load assay and in methodology used in centralized laboratories Abbott M2000, Abbott, USA. The procedure for plasma collection takes less than 10min and in 94% of the cases only one fingerstick was sufficient to collect at least 250μL of blood. The Pearson correlation coefficient value for vp-plasma versus fs-plasma ran on mPIMA was 0.990. The Bland–Altman mean difference (md) for this comparison were virtually zero (md=−0.001) with limits of agreement between −0.225 and 0.223. In addition, the Pearson correlation coefficient value for fs-plasma in mPIMA versus vp-plasma in Abbott M2000 was 0.948 for values above the mPIMA limit of quantification (LoQ; from 800 to 1,000,000copies/mL). These results validate this simple plasma isolation method capable to be implemented in low resource countries where point-of-care decentralization is deeply needed.
HIV viral load (HIV VL) testing is an important tool for monitoring successful anti-retroviral treatment (ART).1 The 90–90–90 HIV targets launched by The Joint United Nations Program on HIV/AIDS (UNAIDS) highlighted the importance of viral load testing and made an urgent call for increased access to viral load and other HIV diagnostic tests.2,3
In developed countries ARV treatment is monitored by VL testing using high throughput standard of care technologies in centralized laboratories. Although centralized testing is a logical solution, it poses a serious challenge in countries where roads are insufficient, many not paved and often blocked by floods. Also challenging are sample collection, cold chain transportation to the central laboratories, and result return to the clinics to aid clinical decision making. In fact, in some settings results take more than one month to return to health professionals and a substantial amount of HIV VL tests fail to return to patient files highlighting the loss of resources and effort.4 For example, in Zimbabwe, use of centralized laboratories for early infant diagnosis resulted in delays of several months for EID diagnosis and nearly half of infants tested never received their results.5
Point-of-care (POC) HIV virus load technologies have been recently developed allowing decentralized HIV VL test to occur. POC assays are simpler and faster than laboratory-based assays, requires minimal training, do not require complex infrastructure and obviates the need for sample transportation. However, they still fall short of expectation by requiring in some cases, large plasma volume (1mL) and needs computer analysis making it cumbersome for some settings. A new POC HIV virus load technology based in thermostable cartridge, mPIMA HIV-1/2 VL (mPIMA), Abbott, USA, has been recently developed. mPIMA HIV-1/2 VL uses a small plasma volume (50μL) with a turnaround time of 1 h, and has a limit of quantification (LoQ) of 800copies/mL and a dynamic range extending up to 106copies/mL. Still, obtaining of 50μL of plasma can be challenging in remote sites or in limited resource settings. In this work, our group validated a simple and reliable way to generate 50μL of plasma from digital puncture blood collection, comparing to venous blood and to M2000 Abbott HIV virus load assay, to be used in settings lacking regular clinical laboratories capable of doing blood collection by venipuncture and regular centrifugation.
MethodsThe mPIMA was evaluated using 50μL of plasma specimens obtained from whole blood collected by venipuncture (vp-plasma) or digital puncture (fingerstick, fs-plasma) from patients with detectable viral load. VL from vp-plasma was first measured by the Abbott M2000 sq and 149/160 specimens with VL falling within the quantitative range of mPIMA (from 800 to 1×106Logcp/mL) were subsequently run on mPIMA. The remaining 11 specimens had VL below 800cp/mL (n=6) or above 106cp/mL (n=5) by Abbott M2000 sq, and were excluded from the evaluation.
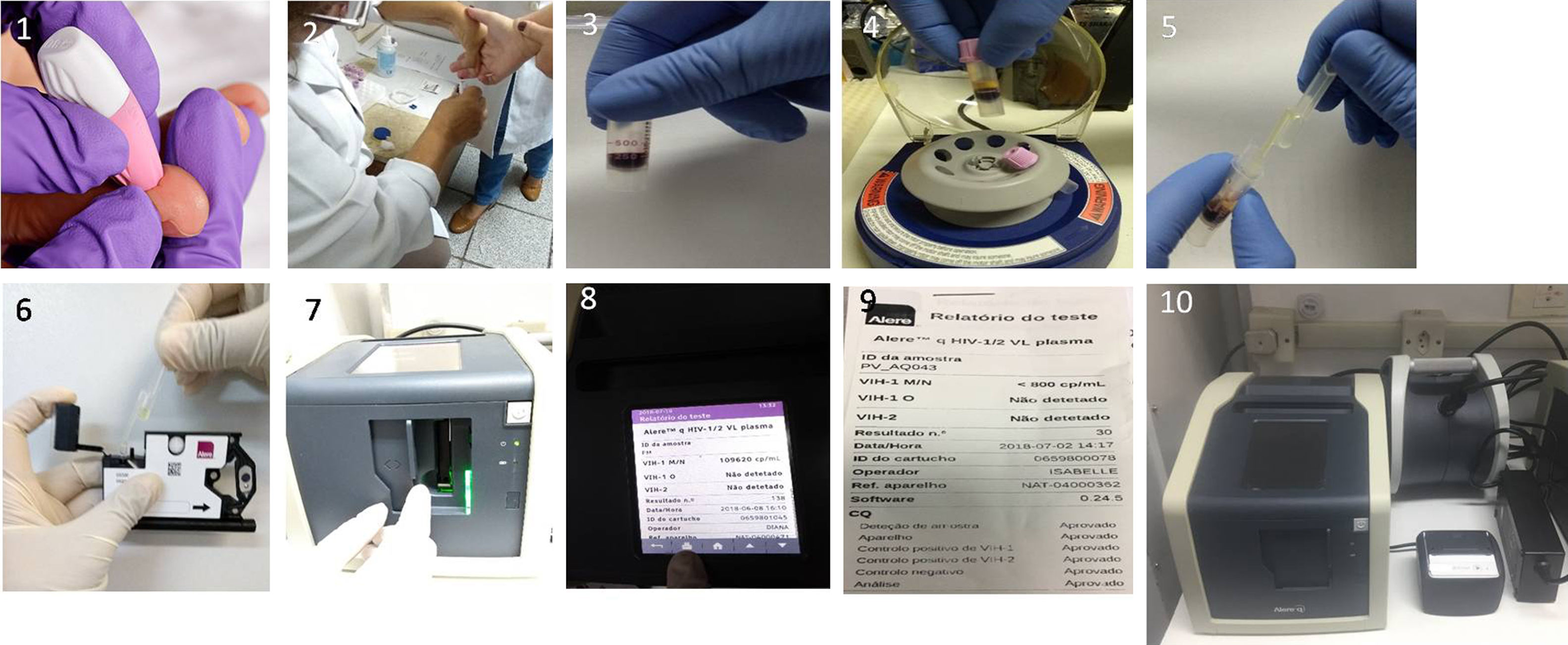
Basically, the mPIMA HIV-1/2 VL plasma test was run following original instructions generating plasma using two different methodologies. The standard procedure was done through venipuncture using an EDTA-Vacutainer tubes followed by centrifugation at 600×g for 10min at room temperature in a regular clinical centrifuge, and 50μL was collected with a regular adjustable volume micropipette. The alternative procedure was developed collecting 250–500μL of blood in an EDTA BD Microtainer tube with BD Microgard (BD Cat# 365974) using a finger stick done with a BD High Flow lancet (BD Cat# 366594). Plasma was separated by centrifuging the microtube at maximum speed for 5min using a 1.5–2.0mL tube microfuge for six tubes (USA Scientific, CAT# 2631-0006) plugged in a computer UPS which gives to the microfuge more than 7h autonomy. After centrifugation 50μL plasma was collected using a fix volume plastic Pasteur pipettes (Pastettes 50μL Dual Bulb, CAT# LW4745-500, Alpha Laboratories Ltd, UK) and added direct on mPIMA cartridge to run (see Fig. 1 and Supplemental Video 1 for more details).

Alternative procedure to generate plasma in sites with no laboratory infrastructure. Each frame represents: 1, fingerstick; 2, collecting the blood flow; 3, blood collected in microtube; 4, minifuge assemble with UPS; 5, collecting plasma with a 50μL fixed volume pippet; 6, loading mPIMA cartridge; 7, inserting the cartridge in mPIMA; 8, result displayed in mPIMA; 9, printing result; 10, full mPIMA apparatus set up.
For this procedure we have established two parameters to measure the feasibility of the method. One was the frequency in which the minimal volume of 250μL of blood from fingerprick collection would be obtained, and second, how many digital puncture would be necessary to obtain such minimal volume.
Results reported in copy number/mL (cp/mL) and were log10 transformed to logcp/mL for statistical analysis. Analysis included agreement between the two assays assessed by the Bland–Altman (B&A) and linear correlation between assays expressed by Pearson correlation coefficient. Analyses were performed with Microsoft Excel software. The results were also compared to Abbott M2000.
This study was ethically reviewed by Hospital GraffeeGuinle IRB under # 86604317.6.0000.5258.
ResultsThe 149 selected specimens that have had plasma obtained by two selection methods (vp-plasma and fs-plasma) were assayed by mPIMA for performance comparison. In parallel, both vp-plasma and fs-plasma were also measured by the Abbott m2000 sq assay.
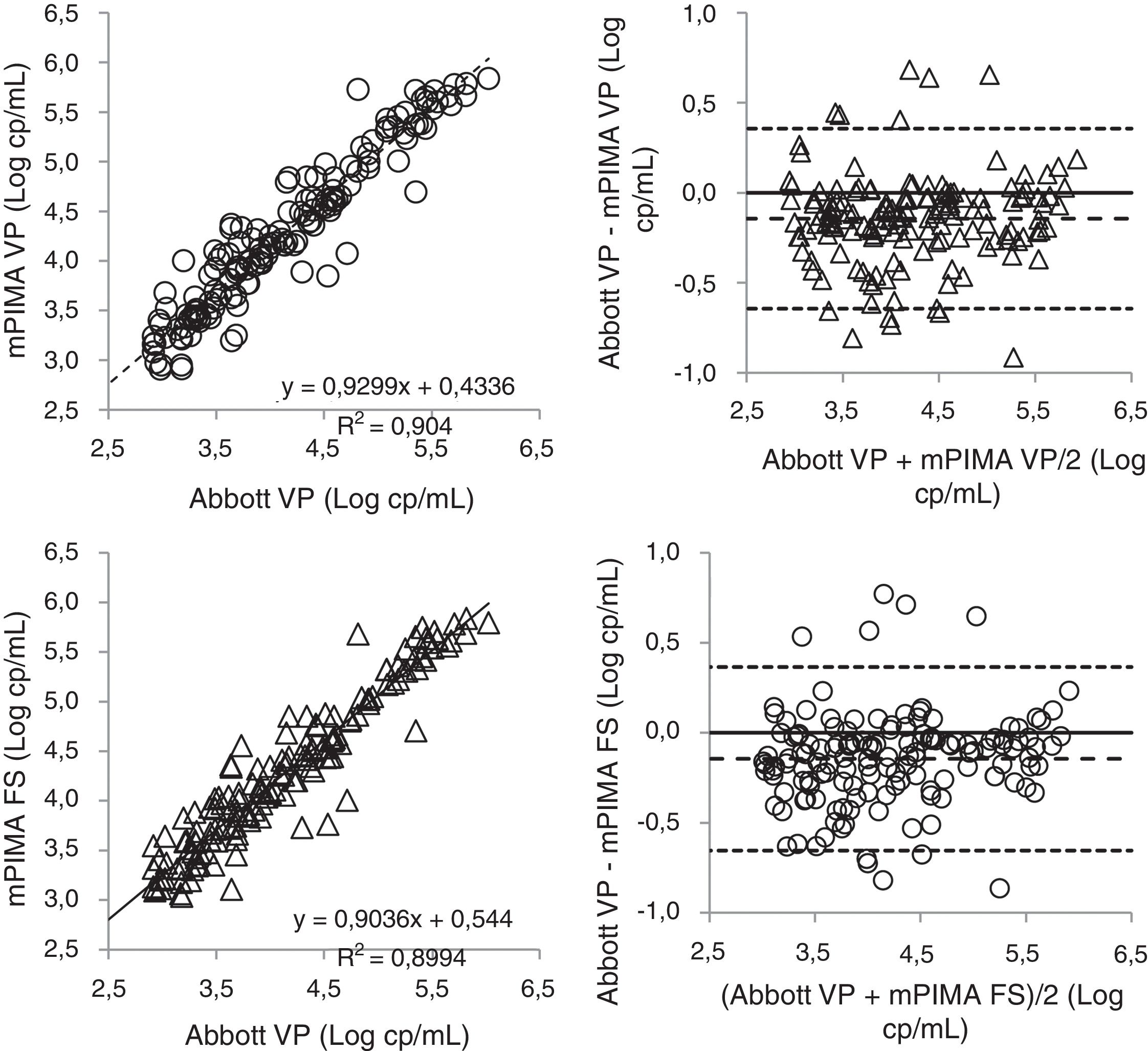
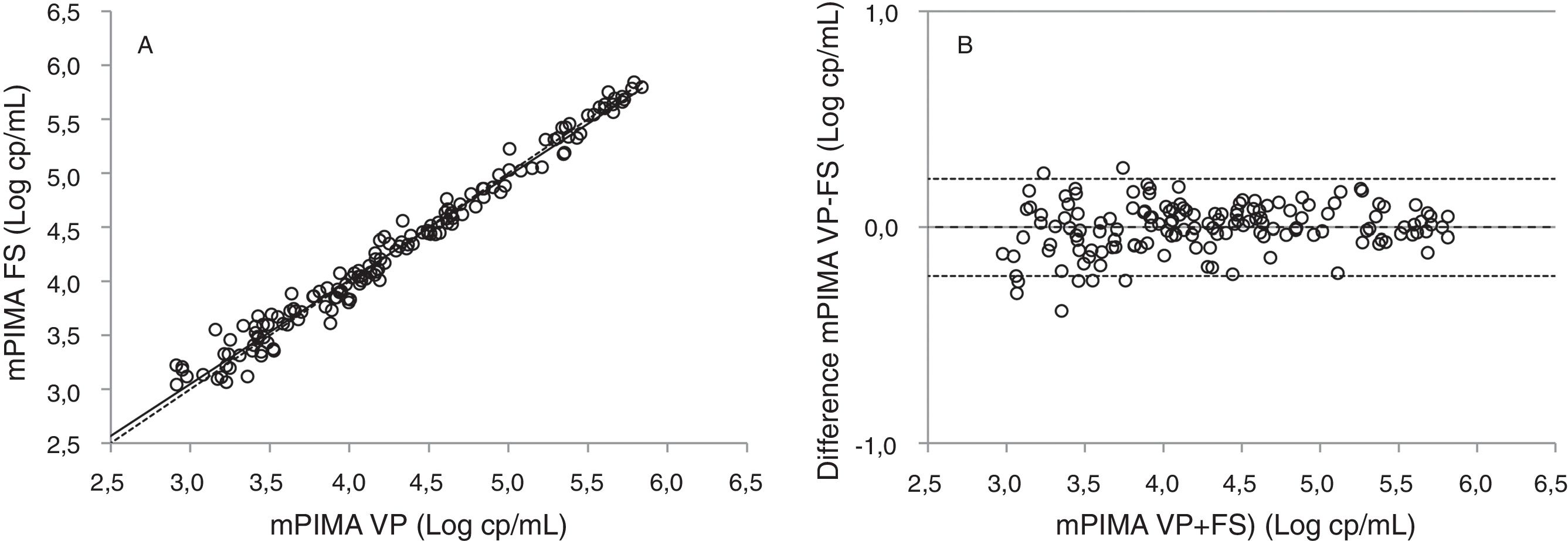
We first looked whether pairs of assay and/or plasma preparation method were linearly correlated. The Pearson correlation coefficient value (R) for each comparison attested a good correlation between pairs, as follows: (a) vp-plasma versus fs-plasma, by mPIMA (R=0.990) (see Fig. 2); (b) vp-plasma by Abbott m2000 versus fs-plasma by mPIMA (R=0.948); and (c) vp-plasma, Abbott m2000 versus mPIMA (R=0.951) (see Fig. 2A and C).
 and (C) show the linear regression and (B) and (D) Bland–Altman analysis, respectively, from VL results using and vp-plasma assayed by Abbott m2000 versus vp-plasma and fs-plasma assayed by mPIMA (n=149 plasma specimens). In (A) and (C), a continuous line shows the LR line. (B) and (D) show the average VL obtained by Abbott vp-plasma minus mPIMA vp-plasma (B) or minus mPIMA fs-plasma (D) versus the VL difference between specimens: dashed line indicates de mean difference between VL of two specimens and dotted lines the limits of agreement of the mean difference. All data shown were log10 transformed.")
(A) and (C) show the linear regression and (B) and (D) Bland–Altman analysis, respectively, from VL results using and vp-plasma assayed by Abbott m2000 versus vp-plasma and fs-plasma assayed by mPIMA (n=149 plasma specimens). In (A) and (C), a continuous line shows the LR line. (B) and (D) show the average VL obtained by Abbott vp-plasma minus mPIMA vp-plasma (B) or minus mPIMA fs-plasma (D) versus the VL difference between specimens: dashed line indicates de mean difference between VL of two specimens and dotted lines the limits of agreement of the mean difference. All data shown were log10 transformed.
We also analyzed level of agreement between pairs of assay and/or plasma preparation method by B&A analysis (Fig. 3). Mean difference (md) and limits of agreement (LoA) were: (a) vp-plasma minus fs-plasma, by mPIMA (md=−0.001; LoA: −0.225 to 0.223); (b) vp-plasma by Abbott m2000 minus fs-plasma by mPIMA (md=−0.145; LoA: −0.655 to 0.365) and; (c) vp-plasma, Abbott m2000 minus mPIMA (md=−0.144; LoA: −0.644 to 0.366) (see Fig. 2B and D).
 and (B) show the linear regression and Bland–Altman analysis, respectively, from VL results using and VP and FS plasma collection methodologies, generated on the mPIMA technology (n=149 plasma specimens). In (A), a continuous line shows the LR analysis and dashed line indicates the equality line. (B) shows the average VL obtained by VP and FS versus the difference between specimens obtained by VP and FS: dashed line indicates de difference (VP-FS) and dotted lines the limits of agreement. All data shown were log10 transformed.")
(A) and (B) show the linear regression and Bland–Altman analysis, respectively, from VL results using and VP and FS plasma collection methodologies, generated on the mPIMA technology (n=149 plasma specimens). In (A), a continuous line shows the LR analysis and dashed line indicates the equality line. (B) shows the average VL obtained by VP and FS versus the difference between specimens obtained by VP and FS: dashed line indicates de difference (VP-FS) and dotted lines the limits of agreement. All data shown were log10 transformed.
Regarding the parameters established to access feasibility of fingerstick blood collection, we have observed that in only one occasion (0.7%) the collected blood volume was less than 250μL. In this particular case, there was no attempt to perform a second fingerstick. Excluding this case, 139/148 (94%) collection yielded blood volume equal to or greater than 250μL, after one single fingerstick. For the last nine individuals, an additional digital puncture was needed to complete the minimal volume. Overall, the procedure takes less than 10min, including when a second digital puncture is needed.
DiscussionThe results generated in this study shown that there are no meaningful VL differences between plasma preparation methods when measurements were done by mPIMA. When the fs-plasma viral load in mPIMA is compared with Abbott M2000, the methodology used until now in centralized laboratories in Brazil, we had an excellent correlation giving a Pearson correlation coefficient value for fs-plasma in mPIMA versus vp-plasma in Abbott M2000 of 0.948 for values above the mPIMA limit of quantification (from 800 to 1,000,000cp/mL). This value for the Pearson correlation coefficient is similar to the one found by Ceffaa et al. (2016) when they compared Abbott M2000 with another methodology (Cepheid GeneXpert). It is important to highlight that Abbott M2000 and other methodologies like GeneXpert need around 1mL of plasma.6 Abbott M2000 assay use 0.6mL of plasma to run, even when adaptations are made, such as for DBS.7
In addition, the collection of 50μL of plasma by fingerstick was feasible and easy to implement in sites without laboratory infrastructure. Of note, VL mean difference between plasma preparation methods was virtually zero (md=−0.001) on samples analyzed by mPIMA.
This performance of plasma obtained by fingerstick (fs-plasma) will make POC HIV VL technology available to follow up and monitor patients under HAART in settings without laboratory infrastructure, like mobile clinics or stand alone outpatient clinics. The use of a UPS linked microfuge makes the plasma separation feasible to be done without the need of regular power source. Using POC VL assays plus the proposed plasma separation methodology could substantially reduce waiting time for viral load results and drastically shorten the time to initiation of ART. Surely, this will impact on HIV transmission in local communities and help countries achieving UNAIDS 90/90/90 target.
FundingThis work was supported by Alere Inc. # FUJB 234/2016.
Conflicts of interestThe authors declare no conflicts of interest.
